ACC317 Application for ACC locum registration (DOC 74K)
advertisement
")
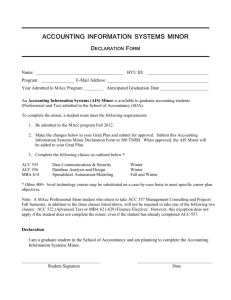
ACC 317 Application for ACC locum registration Use this form to register a locum with ACC. This form was completed on: [dd month yyy] 1. PRACTICE DETAILS Practice name: Practice GST number: Practice street address: Practice postal address (if different from street address): Contact name: Work phone: Preferred method of contact: Contact title: Mobile phone: Work phone Email: Mobile phone Email Post Profession(s): If your locum is an acupuncturist, occupational therapist, chiropractor, physiotherapist, speech therapist, osteopath, podiatrist or audiologist, then indicate the type of payment you require: 2. DETAILS OF CLINICAL Per patient Hourly PROVIDE DETAILS OF EVERYONE USING THIS LOCUM NUMBER PRACTITIONERS Surname First name(s) Annual Practice certificate number Current ACC provider number, if applicable More space is provided at the end of this form. 3. DOCUMENTATION REQUIRED PLEASE ATTACH Please enclose a practice original pre-printed bank deposit slip. We can’t pay you without these details. 4. DECLARATION To be completed and signed by the Senior Practitioner or Practice Manager. I certify that the above information is true and correct, and I confirm that: the practitioners using the number are employed by the practice to provide ad hoc relief work any locum employees using this number are of the same professional group, eg nurses can not use the same number allocated to doctors the number of practitioners registered under one number does not exceed the equivalent of one full time employee ACC is notified, of the name, professional registration number and length of service of any new practitioner due to use the number via the ACC5935 Locum Details Form Name: Job title: Signature: Date: Please return this completed application to: ACC Provider Vendor Registrations, PO Box 30823, Lower Hutt 5040, or email registrations@acc.co.nz ACC317 JUNE 2013 PAGE 1 OF 2 DETAILS OF CLINICAL PRACTITIONERS PROVIDE DETAILS OF ALL CLINICAL USERS OF THIS LOCUM NUMBER Surname Annual Practice certificate number First name(s) Current ACC provider number, if applicable The information collected on this form will only be used to fulfil the requirements of the Accident Compensation Act 2001. In the collection, use and storage of information, ACC will at all times comply with the obligations of the Privacy Act 1993 and the Health Information Privacy Code 1994. ACC317 JUNE 2013 PAGE 2 OF 2