5-6-7-8

Pathogenic bacteriology 2008-2009 Dr. Mahdi AL- Ammar
L( 5) Streptococcus
________________________________________
*Streptococcus pyogenes, other Streptococci, and Enterococcus
*Structure
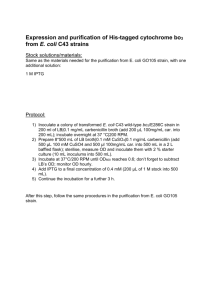
Streptococci are Gram-positive, nonmotile, nonsporeforming, catalase-negative cocci that occur in pairs or chains.
Older cultures may lose their Gram-positive character. Most streptococci are facultative anaerobes, and some are obligate (strict) anaerobes. Most require enriched media (blood agar). Group A streptococci have a hyaluronic acid capsule.
Figure -1 Morphology of the streptococci in comparison with staphylococci .
*Clinical Manifestations
Acute Streptococcus pyogenes infections may take the form of pharyngitis, scarlet fever (rash), impetigo, cellulitis, or erysipelas. *Invasive infections can result in necrotizing fasciitis, myositis and streptococcal toxic shock syndrome. *Patients may also develop immune-mediated sequelae such as acute rheumatic fever and acute glomerulonephritis. *S agalactiae may cause meningitis, neonatal sepsis, and pneumonia in neonates; adults may experience *vaginitis, puerperal fever, urinary tract infection, skin infection, and endocarditis. *Viridans streptococci can cause endocarditis, and Enterococcus is associated with urinary tract and biliary tract infections.
Anaerobic streptococci participate in mixed infections of the abdomen, lungs.
*Classification and Antigenic Types
Streptococci are classified on the basis of colony morphology, hemolysis, biochemical reactions, and (most definitively) serologic specificity. They are divided into three groups by the type of hemolysis on blood agar: bhemolytic (clear, complete lysis of red cells), a hemolytic (incomplete, green hemolysis), and g hemolytic (no hemolysis). Serologic grouping is based on antigenic differences in cell wall carbohydrates (groups A to V), in cell wall pili-associated protein, and in the polysaccharide capsule in group B streptococci.
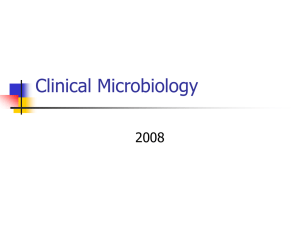
*Pathogenesis figure -2 Cell surface structure of S pyogenes and extracellular substances.
Streptococci are members of the normal flora. Virulence factors of group A streptococci include (1) M protein and lipoteichoic acid for attachment; (2) a hyaluronic acid capsule that inhibits phagocytosis; (3) other extracellular products, such as pyrogenic (erythrogenic) toxin, which causes the rash of scarlet fever; and (4) streptokinase, streptodornase (DNase B), and streptolysins. Some strains are nephritogenic. Immune-mediated sequelae do not reflect dissemination of bacteria. Nongroup A strains have no defined virulence factors .
Figure 2. Pathogenesis of S pyogenes infections.
*Host Defenses
Antibody to M protein gives type-specific immunity to group A streptococci. Antibody to erythrogenic toxin prevents the rash of scarlet fever. Immune mechanisms are important in the pathogenesis of acute rheumatic fever.
Maternal IgG protects the neonate against group B streptococci.
*Epidemiology
Group A ?-hemolytic streptococci are spread by respiratory secretions and fomites. The incidence of both respiratory and skin infections peaks in childhood. Infection can be transmitted by asymptomatic carriers .
*Diagnosis
Diagnosis is based on cultures from clinical specimens. Serologic methods can detect group A or B antigen; definitive antigen identification is by the precipitin test. Bacitracin sensitivity presumptively differentiates group A from other b-hemolytic streptococci (B, C, G.;)
*Control
Prompt penicillin treatment of streptococcal pharyngitis reduces the antigenic stimulus and therefore prevents glomerulonephritis and acute rheumatic fever. Vancomycin resistance among the enterococci is an emerging microbial threat. Vaccines are under development.
*Streptococcus pneumoniae
*Clinical Manifestations
S pneumoniae causes pneumonia, meningitis, and sometimes occult bacteremia.
*Structure
Pneumococci are lancet-shaped, catalase-negative, capsule-forming, -hemolytic cocci or diplococci. Autolysis is enhanced by adding bile salts.
*Classification and Antigenic Types
There are more than 85 antigenic types of S pneumoniae, which are determined by capsule antigens. There is no
Lancefield group antigen.
*Pathogenesis
S pneumoniae is a normal member of the respiratory tract flora; invasion results in pneumonia. The best defined virulence factor is the polysaccharide capsule, which protects the bacterium against phagocytosis .
Figure 13-4 Pathogenesis of S pneumoniae infections.
*Host Defenses
Protection against infection depends on a normal mucociliary barrier and intact phagocytic and T-independent immune responses. Type-specific anti-capsule antibody is protective.
*Diagnosis
Diagnosis is based on a sputum Gram stain and culture; blood or cerebrospinal fluid may also be cultured.
Capsular antigen can be detected serologically. Pneumococci are distinguished from viridans streptococci by the quellung (capsular swelling) reaction, bile solubility, and optochin inhibition.
Control
Treatment is usually with penicillin. However, strains resistant to penicillin and multiple antibiotics are rapidly emerging. A vaccine is available.
Pathogenic Bacteriology Kufa University
4-th-Years Collage of science
Dr.Mahdi Al Ammar Dpt. of Biology
Gram-Negative Rods (Enterobacteriaceae)Lec( 6 )
* Introduction
The Enterobacteriaceae are a large, heterogeneous group of gram-negative rods whose natural habitat is the intestinal tract of humans and animals. The family includes many genera ( Escherichia, Shigella, Salmonella,
Enterobacter, Klebsiella, Serratia, Proteus, and others). , Escherichia coli, are part of the normal flora and incidentally cause disease, while , the salmonellae and shigellae, are regularly pathogenic for humans. *The
Enterobacteriaceae are facultative anaerobes or aerobes,* ferment a wide range of carbohydrates,* possess a complex antigenic structure, and *produce a variety of toxins and other virulence factors.
* Classification
The family Enterobacteriaceae have the following characteristics: 1.They are gram-negative rods, 2.either motile with peritrichous flagella or nonmotile; 3.they grow on peptone or meat extract media without the addition of sodium chloride or other supplements;4. grow well on
MacConkey's agar; 5..grow aerobically and anaerobically (are facultative anaerobes); 6.ferment rather than oxidize glucose, often with gas production; 7.are catalase-positive, oxidase-negative, and reduce nitrate to nitrite; and 8. have a 39–59% G + C DNA content.
*Morphology & Identification
The Enterobacteriaceae are short gram-negative rods. Typical morphology is seen in growth on
solid media in vitro, but morphology is highly variable in clinical specimens. Capsules are large and regular in klebsiella, *Culture
1.E coli and most of the other enteric bacteria form circular, convex, smooth colonies with distinct edges. 2.Enterobacter colonies are similar but somewhat more mucoid. 3.Klebsiella colonies are large and very mucoid 4. The salmonellae and shigellae produce colonies similar to
E coli but do not ferment lactose. 5.Some strains of E coli produce hemolysis on blood agar.
* Growth Characteristics a).Carbohydrate fermentation and (b).the activity of amino acid decarboxylases and (c). enzymes are used in biochemical differentiation . Some tests , eg, the (a).production of indole from tryptophan, while ( b. )the Voges-Proskauer reaction (production of acetylmethylcarbinol from dextrose), are used. *Culture on "differential" media (eg, eosin-methylene blue [EMB],
MacConkey's, or deoxycholate medium) distinguishes lactose-fermenting from non-lactosefermenting colonies (Table –1).
Table 1. Rapid, Presumptive Identification of Gram-Negative Enteric Bacteria.
*Lactose Fermented Rapidly
Escherichia coli: metallic sheen on differential media; motile; flat, nonviscous colonies
Enterobacter aerogenes: raised colonies, no metallic sheen; often motile; more viscous growth
Klebsiella pneumoniae: very viscous, mucoid growth; nonmotile
*Lactose Fermented Slowly
Serratia, Citrobacter, Arizona,
*Lactose Not Fermented
Shigella species: nonmotile; no gas from dextrose
Salmonella species: motile; acid and usually gas from dextrose
Proteus species: "swarming" on agar; urea rapidly hydrolyzed (smell of ammonia)
Pseudomonas species: soluble pigments, blue-green and fluorescing; sweetish smell
A complex media have been devised to help in identification of the enteric bacteria.A. Triple sugar iron (TSI) agar, which is used to help differentiate salmonellae and shigellae from other enteric gram-negative rods in stool . B.If only glucose is fermented,. If lactose or sucrose is fermented, so much acid is produced that the slant and butt remain yellow (acid). Salmonellae and shigellae typically yield an alkaline slant and an acid butt. Although proteus, providencia, and morganella produce an alkaline slant and acid butt, they can be identified by their rapid formation of red color in Christensen's urea medium. Organisms producing acid on the slant and acid and gas (bubbles) in the butt are other enteric bacteria.
* Escherichia
E coli positive indole, lysine decarboxylase, and mannitol fermentation and produces gas from glucose. E coli its hemolysis on blood agar, typical colonial morphology with an iridescent
"sheen" on differential media such as EMB agar,-
*Klebsiella-Enterobacter-Serratia Group
The coliforms and Proteus are Gram negative bacilli. All genera except Klebsiella are flagellated. Some strains produce capsules. Virulence often depends on the presence of
attachment pili . Sex pili also may be present Sex pili, genetically determined by extrachromosomal plasmids, in coliforms and Proteus sp.the sex pili are involved in genetic transfer by conjugation .
.
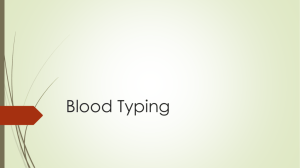
* Major Surface Antigens ( Antigenic Structure)
The Ags of coliforms are referred to as H, K, and O antigens. E coli, Enterobacter, Serratia,
Citrobacter, and Proteus organisms are peritrichous flagella . Klebsiella sp. are nonmotile and nonflagellated and have no H Ags.
Fig-1 Structure and antigenic composition of coliforms and Proteus species.
The outer membrane of the bacterial cell wall of these species contains receptors for bacterial viruses and bacteriocins . The outer membrane also contains lipopolysaccharide (LPS), of which the lipid A portion is endotoxic and the O (somatic) antigen is serotype specific.
1.O antigens are the external part of the cell wall lipopolysaccharide and consist of repeating units of polysaccharide. O antigens are resistant to heat and alcohol and detected by bacterial agglutination. Antibodies to O antigens are IgM. O antigens may be associated with diarrhea and in urinary tract infections.
2.K antigens K antigens (capsule polysacchride) . K antigens of E coli are pilus-like proteins.
The K antigens block agglutination by specific O antisera ; . K antigens may interfere with agglutination by O antisera, and associated with virulence (g, E coli producing K1 antigen are prominent in meningitis, and K antigens of E coli cause attachment of the bacteria to epithelial cells prior to gastrointestinal or urinary tract invasion).
Klebsiellae form polysaccharides (K antigens) covering the somatic (O or H) antigens and can be identified by capsular swelling tests . Citrobacter produce Vi (virulence) antigen, a K antigen also found in Salmonella typhi.
3.H antigens are located on flagella and are removed by heat or alcohol. H antigens agglutinate
with anti-H antibodies, mainly IgG. H –Ag are flagellar protein (flagellin).
*Pathogenesis : a).E coli strains isolated from extraintestinal infections often possess a number of properties .
These include production of soluble and cell-bound hemolysins, the colicin V plasmid, production of the siderophores aerobactin and enterochelin, and special pilial Ags for adherence to target cells. (b)The hemolysin kills host cells and makes iron more available by releasing hemoglobin-bound iron from lysed red cells. (c), E coli produces siderophores of both the hydroxamate (aerobactin) and phenolate (enterochelin) types.(d) Common pili may mediate adherence to bladder cells;
(e)The urease, produced by Proteus, and lesser by Klebsiella sp. is play a role in the production of infection-induced urinary stones. Urease hydrolyzes urea to ammonia and Co2..
* Biochemical tests .
Klebsiella * exhibit mucoid growth, *large polysaccharide capsules, *and lack of motility, It positive tests for lysine decarboxylase and citrate . Enterobacter is positive for motility, citrate, and ornithine decarboxylase and produce gas from glucose. * Enterobacter aerogenes has small capsules. Serratia produces DNase, lipase, and gelatinase. Kl., enterobacter, and serratia are positive Voges-Proskauer reactions.
*Proteus-
are motile, grow on (KCN), and ferment xylose. Proteus species move very actively by means of peritrichous flagella, resulting in "swarming" on solid media . Proteus sp. are urease-positive,
. . Proteus mirabilis is more susceptible to antimicrobial drugs, including penicillins, .
*Citrobacter: These bacteria are citrate-positive and differ from the salmonellae in that they do not decarboxylate lysine. .
*Salmonella : Salmonellae are motile rods that characteristically ferment glucose and mannose without producing gas but do not ferment lactose or sucrose. Most salmonellae produce H
2
S.
They are often pathogenic for humans or animals when ingested.
*Colicins (Bacteriocins) :(plasmid-encoded, antibiotic like bactericidal proteins called colicins in E coli that are active against the same or closely related species).Many gram-negative organisms produce bacteriocins. Their production is controlled by plasmids. Colicins are produced by E coli, marcescens by serratia, and pyocins by pseudomonas.
*Toxins & Enzymes
Most gram-negative bacteria possess lipopolysaccharides in their cell walls. , endotoxins, .
Many gram-negative enteric bacteria also produce exotoxins .
Pathogenic Bacteriology Kufa University
4-th-Years Collage of science
Dr.Mahdi Al Ammar Dpt. of Biology
Lec( 7 )
*Causative Organisms of Enterobacterace
1.E coli is and other enteric bacteria ( Proteus, Enterobacter, Klebsiella, Morganella, Providencia,
Citrobacter, and Serratia species) are found as members of the normal intestinal flora but are less than E coli.
2.The enteric bacteria are found as part of the normal flora of the upper respiratory and genital tracts.3. The enteric bacteria in the intestine contribute to normal function and nutrition.. 4.The bacteria become pathogenic when they reach tissues ..
*Pathogenesis & Clinical Findings
1.E colI :
* Urinary Tract Infection
E coli is cause of urinary tract infection . The symptoms and signs include y, dysuria, hematuria, and pyuria.
Nephropathogenic E coli produce a hemolysin( O & K antigen)is important in the pathogenesis of upper tract infection. Pyelonephritis is associated with pilus, P pilus,
*E coli-Associated Diarrheal Diseases
E coli are cause diarrhea . The small or large bowel epithelial cell adherence properties are encoded by genes on plasmids. .
1.Enteropathogenic E coli (EPEC) is an important cause of diarrhea in infants, . EPEC adhere to the mucosal cells of the small bowel. The result of EPEC infection is watery diarrhea, which associated with E coli; are identified by O& H antigen typing..
2.Enterotoxigenic E coli (ETEC) is cause of "traveler's diarrhea" . ETEC colonization factors promote adherence of ETEC to epithelial cells of the small bowel. Some of ETEC produce a heat-labile exotoxin .
Some of ETEC produce the heat-stable enterotoxin ST a
The plasmids carrying the genes for enterotoxins (LT, ST) also may carry genes for the colonization factors that facilitate the attachment of E coli strains to intestinal epithelium.
3.Enterohemorrhagic
E coli (EHEC) produces verotoxin, its cytotoxic effect on Vero cells, . EHEC has been associated with hemorrhagic colitis, Verotoxin are similar to the Shiga toxin /
4.Enteroinvasive
E coli (EIEC) produces a disease very similar to shigellosis. The disease occurs in children . Like shigella, EIEC strains are nonlactose or late lactose fermenters and are nonmotile. .
5.Enteroaggregative
E coli (EAEC) causes acute and chronic diarrhea ... EAEC produce ST-like toxin and
a hemolysin.
* Sepsis : When , E coli reach the bloodstream and cause sepsis.
* Meningitis ; E coli causes of meningitis in infants.that have the K1 antigen.
2.
Klebsiella
K pneumoniae is present in the respiratory tract and feces .
K pneumoniae can produce hemorrhagic necrotizing of the lung. It produces urinary tract infection and bacteremia . Klebsiella ozaenae has been isolated from the nasal mucosa in ozena, a fetid, .
3.Enterobacter aerogenes
This organism has small capsules, may be found free-living as well as in the intestinal tract, and causes urinary tract infections and sepsis.
4.Serratia
Serratia causes pneumonia, bacteremia, and endocarditis in hospitalized patients. . S marcescens is multiply resistant to aminoglycosides and penicillins; infections can be treated with third-generation cephalosporins.
5.Proteus
Proteus produce infections in humans only when the bacteria leave the intestinal tract. They are found in urinary tract infections and produce bacteremia, pneumonia, .
Proteus sp produce urease, resulting in hydrolysis of urea with liberation of ammonia. , the urine becomes alkaline, promoting stone formation and making acidification . The rapid motility of proteus may contribute to its invasion of the urinary tract.
P mirabilis is inhibited by penicillins; active antibiotics are aminoglycosides and cephalosporins.
* Diagnostic Laboratory Tests
*Specimens:Specimens included urine, blood, pus, spinal fluid, sputum,
*Culture: Specimens are plated on both blood agar and differential media.
*Immunity:Specific antibodies develop in systemic infections, .
*Treatment: . The sulfonamides, ampicillin, cephalosporins, fluoroquinolones, and aminoglycosides have antibacterial effects against the enterics,.
6.The Shigellae :
* Morphology & Identification : Shigellae are slender gram-negative rods; coccobacillary forms occur in young cultures. nonmotile, facultatively anaerobic, non-spore-forming rods
.Shigellae do not ferment lactose and others carbohydrates, producing acid but not gas. do not produce H
2
S. The four Shigella species are closely related to E coli.
.
The shigellae is limited to the intestinal tracts of humans and other primates, where they produce bacillary dysentery.
*Culture : Shigellae are Convex, circular, transparent colonies with intact edges reach a
diameter of about 2 mm in 24 hours.
*Growth Characteristics :
All shigellae ferment glucose exception of Sh. sonnei, . Shigellae form acid from carbohydrates but rarely produce gas. S dysenteriae negative but, S flexneri , S sonnei are postive Mannitol .the S.dysenteriae
& S flexneri are nagative but S sonnei is posative decarboxylase.
*Antigenic Structure :The somatic O antigens of shigellae are LPS.
*Pathogenesis & Pathology :Infection is initiated by ingestion of shigellae ( fecal-oral contamination). An early symptom, diarrhea ( elicited by enterotoxins and/or cytotoxin), may occur as the organisms pass through the small intestine. Colitis in the rectosigmoid mucosa, with concomitant malabsorption, results in the characteristic sign of bacillary dysentery: scanty,. unformed stools tinged with blood and mucus.
Shigella infections are limited to the gastrointestinal tract; bloodstream invasion is quite rare. the infective dose is on the order of 10
3
organisms . the pathologic process is invasion of the mucosal epithelial cells by *induced phagocytosis,* escape from the phagocytic vacuole, *multiplication and spread within the epithelial cytoplasm, and* passage to adjacent cells..
* Pathology: Shigella infection is initiated at the membranous (M) cells that are associated with macroscopic lymphoid follicles (Peyer's patches). During the early stages of infection, bacteria are transcytosed through the M cells into the subepithelial space. In the subepithelial space, the organisms are phagocytosed by resident macrophages. However, virulent shigellae are not killed and digested in the macrophage phagolysome. The bacteria lyse the phagosome and initiate apoptosis (programmed cell death). During this process, the infected macrophage releases the inflammatory cytokine IL-1, which elicits infiltration of PMN.
*Histopathology of acute colitis following infection with shigellae.
* Endotoxin ; all shigellae release their toxic lipopolysaccharide. These virulence determinants are encoded by large extra-chromosomal (plasmids) that are functionally identical in all Shigella sp. and in EIEC.
*Shigella dysenteriae Exotoxin
S dysenteriae produces a heat-labile exotoxin that affects both the gut and the central nervous system. is antigenic and lethal for animals. Acting as an enterotoxin, it produces diarrhea as the E coli verotoxin, . Acting as a," . The toxin producing an early nonbloody, diarrhea and the invasion of the large intestine resulting in later dysentery with blood and pus in stools.
*Clinical Findings
Shigellosis has 2-basic clinical (1) watery diarrhea associated with vomiting and mild moderate dehydration, (2) dysentery characterized by a small volume of bloody,mucoid stools, and abdominal pain(cramps and tenesmus.After a short incubation period (1–2 days), there is a sudden onset of abdominal pain, fever, and watery diarrhea. As the infection involves the ileum and colon, the number of stools increases; and contain mucus and blood.
*Host defense : Serotype-specific immunity is induced by a primary infection, suggesting a protective role of antibody recognizing the (LPS) . Other Shigella antigens include enterotoxins, cytotoxin, and plasmid-encoded proteins that induce bacterial invasion of the epithelium. Injection of killed shigellae stimulates production of antibodies in serum but fails to protect humans against infection. IgA in the gut limiting reinfection; by live attenuated given orally as vaccines. Serum Ab to O- shigella Ags are IgM.
*Diagnostic : Specimens include fresh stool, mucus flecks, and rectal swabs. *Culture: The materials are streaked on differential media (eg, MacConkey's or EMB agar) and on selective media (Hektoen enteric agar or salmonella-shigella agar), which suppress other
Enterobacteriaceae and gram-positive organisms. (lactose-negative) colonies are inoculated into triple sugar iron agar. Not produce H
2
S, that produce acid but not gas in the butt and an alkaline slant in triple sugar iron agar medium, and nonmotile ,it agglutination by specific
shigella antisera.
*Treatment: Ciprofloxacin, ampicillin, doxycycline, and trimethoprim-sulfamethoxazole are most commonly inhibitory for shigella isolates .
Pathogenic Bacteriology
Kufa University
4-th-Years Collage of science
Dr.Mahdi Al Ammar Dpt. of Biology
Lec( 8 ) 2009-2009
(C).The Salmonella
Salmonellae are often pathogenic for humans or animals when acquired by the oral route. They are transmitted from animals and animal products to humans, where they cause enteritis, systemic infection, and enteric fever. Salmonellae are Gram-negative, flagellated, facultatively anaerobic bacilli possessing three major antigens: H or flagellar antigen; O or somatic antigen; and Vi Ag.
*Morphology & Identification
* Most isolates are motile with peritrichous flagella.* Salmonellae grow readily on simple media, but not ferment lactose or sucrose. *They form acid and sometimes gas from glucose and mannose. *They usually produce H
2
S. They survive in water . Salmonellae are resistant to (eg, brilliant green, sodium tetrathionate, sodium deoxycholate) that inhibit other enteric bacteria;
*Pathogenesis & Clinical Findings
Salmonellae must possess a variety of attributes called virulence factors. These include (1) the ability to invade cells, (2) a complete lipopolysaccharide coat, (3) the ability to replicate intracellularly, and (4) possibly the elaboration of toxin(s). After ingestion, the organisms colonize the ileum and colon, invade the intestinal epithelium, and proliferate within the epithelium and lymphoid follicles Salmonellosis includes several syndromes (gastroenteritis, enteric fevers, septicemia, focal infections, and an asymptomatic carrier state)
After invading the epithelium, the organisms multiply intracellularly and then spread to mesenteric lymph nodes and body via the systemic circulation; . The reticuloendothelial system confines and controls spread of the organism. , some organisms may infect the liver, spleen, gallbladder, bones, meninges, and other organs.
After invading the intestine, most salmonellae induce an acute inflammatory response, which can cause ulceration. They may elaborate cytotoxins that inhibit protein synthesis. However, invasion of the mucosa causes the epithelial cells to synthesize and release various proinflammatory cytokines, including: IL-1, IL-
6, IL-8, TNF-2, IFN-U, MCP-1, and GM-CSF. These evoke an acute inflammatory response and may also be responsible for damage to the intestine. the, symptoms of inflammation such as fever, chills, abdominal pain, leukocytosis, and diarrhea are common. The stools may contain polymorphonuclear leukocytes, blood, and mucus. the diarrhea is due to secretion of fluid and electrolytes by the small and large intestines. . Salmonella penetrate the intestinal epithelial cells . Salmonella escape from the basal side of epithelial cells into the lamina propria. Systemic spread of the organisms can occur, giving rise to enteric fever. Invasion of the intestinal mucosa is followed by activation of mucosal adenylate cyclase; the resultant increase in cyclic
AMP induces secretion. .
Figure-2 Scheme of the Pathogenesis of Salmonella enterocolitis and diarrhea.
Figure -3 Invasion of intestinal mucosa by Salmonella.
Salmonella Typhi, Salmonella Choleraesuis, and perhaps Salmonella Paratyphi A and Salmonella Paratyphi
B are primarily infective for humans.
The organisms enter via the oral route, with contaminated food or drink. The infective dose is 10
5 –10 8
.
Salmonellae produce three main types of disease in humans, but mixed forms are frequent (Table –5).
Table –5. Clinical Diseases Induced by Salmonellae.
Incubation
Onset
Enteric Fevers
7–20 days
Insidious
Septicemias
Variable
Abrupt
Enterocolitis
8–48 hours
Abrupt
Fever Gradual,, with "typhoidal" Rapid rise, then Low state "septic"Temp
Duration of disease Several weeks Variable 2–5 days
Gastrointestin symptoms
Blood cultures
early constipation; later, None bloody diarrhea
Nausea, vomiting, diarrhea at onset
Stool cultures
Positive in first to second Positive during high Negative weeks fever
Positive from 2nd week on; Positive Positive soon after onset
*The "Enteric Fevers" (Typhoid Fever )
This syndrome is produced by Salmonella Typhi (typhoid fever) . The ingested salmonellae reach the small intestine, which they enter the lymphatics and then the bloodstream. They are carried by the blood to many organs, including the intestine. The organisms multiply in intestinal lymphoid tissue and are excreted in stools.
*After an incubation period of 10–14 days,1. fever, malaise, headache, constipation, bradycardia, and myalgia occur. 2.The fever rises , 3.and the spleen and liver become enlarged.4. Rose spots, on the skin of the abdomen or chest, .
*Bacteremia & *Enterocolitis
Eenterocolitis can be caused by any of the more than 1400 group I serotypes of salmonellae. 8-to 48 hours after ingestion of salmonellae, there is nausea, headache, vomiting, and profuse diarrhea, with few leukocytes in the stools.
*Endotoxin
Salmonellae contains a complex lipopolysaccharide (LPS) structure that is liberated on lysis of the cell , during culture. The lipopolysaccharide may be function as an endotoxin, and may be important in virulence
. This endotoxin complex consists of three components, an outer O-polysaccharide coat, a middle portion
(the R core), and an inner lipid A coat. Lipopolysaccharide structure is important for several reasons. First, the nature of the repeating sugar units in the outer O-polysaccharide chains is responsible for O antigen specificity; it may also help determine the virulence of the organism. Second, antibodies directed against the
R core may protect against infection by a wide variety of Gram-negative bacteria . Third , the endotoxin may play an important role in the pathogenesis of Gram-negative infections. Endotoxins evoke fever, activate the serum complement, kinin, and clotting systems, , and alter lymphocyte function.
*Diagnostic Laboratory Tests:*Specimens
Blood cultures are positive in the first week . Bone marrow,. Urine & stool cultures may be positive after the second week, ; in enterocolitis, during the first week.
* Methods for Isolation of Salmonellae
*Differential Medium : EMB, MacConkey's, or deoxycholate medium permits rapid detection of lactose
nonfermenters . Many salmonellae produce H
2
S.
*Selective Medium Cultures: (SS) agar, Hektoen enteric agar, XLD, or deoxycholate-citrate agar,.
*Enrichment :The specimen (usually stool) also is put into selenite F or tetrathionate broth, which inhibit replication of normal intestinal bacteria .
* Identification:Suspect colonies are identified by biochemical reaction.
*Serologic Methods: may be used to determine antibody titers in patients .
A-Agglutination Test
B-Tube Dilution Agglutination Test (Widal Test)
The Widal test to detect these antibodies against the O and H antigens .
*Immunity
Secretory IgA antibodies may prevent attachment of salmonellae to intestinal epithelium.
*Treatment
Antimicrobial therapy of invasive salmonella infections is with ampicillin, trimethoprim-sulfamethoxazole, or a third-generation cephalosporin. given significant protection in areas of high endemicity. Vaccines against other salmonellae give less protection and are not recommended. Structure,