Bells Palsy - Swansea Acute GP Services homepage
advertisement

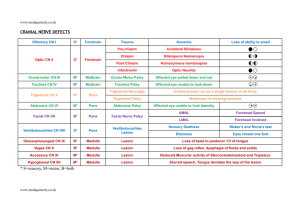
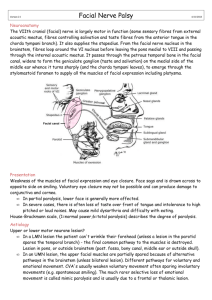
Bells Palsy Acute unilateral facial nerve palsy. Patients with Bell's palsy can be managed in the community. They can be assessed next day in Singleto ENT Clinic after discussion with ENT Differential diagnosis includes stroke and Ramsay-Hunt syndrome (see below). If diagnostic doubt remains the patient can be referred to the next TIA clinic for a consultant opinion. Differential diagnosis "It is important to identify whether the patient has an upper motor neurone (UMN) or lower motor neurone (LMN) lesion to assist in identifying cause. In a LMN lesion [e.g. Bell's palsy] the patient can't wrinkle their forehead - the final common pathway to the muscles is destroyed. Lesion must be either in the pons, or outside the brainstem (posterior fossa, bony canal, middle ear or outside skull). In an UMN lesion [e.g. stroke], the upper facial muscles are partially spared because of alternative pathways in the brainstem i.e. the patient can wrinkle their forehead (unless bilateral lesion) and the sagging of the face seen with lower motor neurone palsies is not as prominent. There appear to be different pathways for voluntary and emotional movement. CVA's usually weaken voluntary movement often sparing involuntary movements (e.g. spontaneous smiling). The much rarer selective loss of emotional movement is called mimic paralysis and is usually due to a frontal or thalamic lesion." Give patient information from PatientUK Ramsay Hunt syndrome. Lower motor neuron facial palsy may be due to Varicella zoster virus (VZV) reactivation. The following additional symptoms may suggest VZV: deafness dizziness vertigo vesicles, often in pharynx and ear, but sometimes there is no rash Consider treatment with high dose antivirals e.g. acyclovir (first line). Treatment must be started within 48 hours of onset. Treatment of Bell's palsy Treatment with high dose oral steroids does improve the complete facial recovery rate if given within 3 days of onset. . Adult Bell’s palsy : Start Prednisolone 1mg / kg body weight per day (a maximum of 60mg) for a week if no contraindications & Aciclovir 400mg 5 times a day for a week if seen within 3 days of onset. Consider artificial tears and taping closed eyelid to protect cornea.