Paediatric Bell’s Palsy
Paediatric Update
November 2014
Richard Webster,
Paediatric Neurologist
Children’s Hospital at Westmead
Typical history
Unilateral LMN facial weakness
Acute onset
– over a day or two
– progressive worst within 2-4 weeks
Preceding ear canal pain
Recovery of function
– starts within 3 weeks
– resolution within 6 months
Definition Bell’s palsy
Acute idiopathic peripheral facial
nerve palsy
– 1. Assessment
– 2. Differential diagnosis
– 3. Treatment
– 4. Monitoring
..but first some anatomy
Facial nerve motor nucleus
– Lower pons
– Fibres of VIn curve around the VIIn nucleus
– Bilateral supranuclear inputs for upper
face control
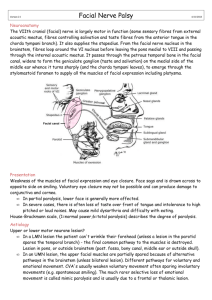
Facial nerve
– Leaves pontomedullary junction
– Sensory/autonomic fibres join in facial canal
– Passes through the facial canal
Facial nerve anatomy
Functions of facial nerve
– 1. Facial expression
– 2. Lacrimal gland – greater petrosal
nerve
– 3. Nerve to stapedius
– 4. Taste fibres to anterior 2/3 tongue
(chorda tympani)
– 5. Sensation external auditory meatus
– 6. Salivation – (chorda tympani)
1. Assessment: facial expression
1. Observe
2. Look up
3. Eye closure
4. Muscles of facial expression
– Smile – emotional/voluntary
– Blow out cheeks – lip closure
5. Platysma
– Difficult
Bell’s palsy algorithm?
Facial palsy?
LMN
UMN
Face assessment
1. What is weak?
– One side or both sides
– Is it all consistent with VIIn?
2. Is the forehead involved?
– UMN lesions spare the forehead
– Get the child to look up
1. Where in the nerve is
the lesions?
1. Dry eye?
2. Hyperacusis?
3. Loss of taste (difficult in most
children) ant 2/3 of tongue
4. Test for auricular sensation
Bell’s palsy algorithm
Facial palsy?
LMN
UMN
Neurological exam
Isolated
Other signs
Is this isolated facial n
palsy?
Cranial nerves
– II – papilloedema
– VI + gaze – nuclear lesions
– VIII – hearing
– IX, X – swallowing, palate
– XI,XII
Cerebellum
Long tract signs
Gait
Neurological differential
diagnosis
1. Nerve disease
– Infiltration
– Inflammation/infection
– Compression – bone/neoplasm
2. Muscle disease
– Myasthenia
Case
8 yo girl with R LMN VII weakness
– Gradual onset
Treated with steroids for 1/52 no
improvement then given a second course
No improvement within 3 weeks
Then developed unsteady gait
– Limitation of eye movement to right
– Deviates to right on tandem gait
Bell’s palsy algorithm
Facial palsy?
LMN
UMN
Neurological exam
Isolated
Examination/Ix
No cause
Other signs
BP - hypertension
FBC - leukaemia
Middle EarOM/mastoiditis,
Herpes
Further examination
Check ears
– ? Otitis media
– ? Evidence of vesicles (Ramsay Hunt)
Systemic examination
– BP
– Hepato-splenomegaly/pallor
FBC – evidence of leukaemia
Warning signs
Young age
Bell’s palsy uncommon in infants and
young children
3/100,000 < 10, 25/100,00 adults
Malignancy/ diseases predisposing to
malignancy
History of recurrent otitis media
Syndromes associated with facial
dysmorphism
Bell’s palsy algorithm
Facial palsy?
LMN
UMN
Neurological exam
Isolated
Other signs
Examination/Ix
No cause
Treat
BP - hypertension
FBC - leukaemia
Middle EarOM/mastoiditis,
Herpes
3. Treatment
Eye protection
– Avoid corneal abrasions if the patient with
facial palsy is unable to close the eye.
– Artificial tears during the day
– Ointment at night
– Eye patch if needed
Treatment
Steroids
– No definite evidence but strong
adult data
– Prednisolone 2mg/kg/day (max 6080mg)
– Give for 5 days and then taper for 5
days
– (Up to date)
Bell’s palsy algorithm
Facial palsy?
LMN
UMN
Neurological exam
Isolated
Other signs
Examination
No cause
Treat
Review
BP - hypertension
FBC - leukaemia
Middle EarOM/mastoiditis,
Herpes
4. When to review?
Review
– 1 week after diagnosis
– Weekly until clear improvement
– Follow-up to make sure of resolution
Imaging/referral
Unusual history
– Slow onset
Progression beyond 3 weeks
Failure to improve after 4 weeks
Associated history/signs
suggesting a more sinister cause
for Bell’s palsy
 0
0