SIMULATION OF THE RADIOGRAPHY FORMATION PROCESS
advertisement

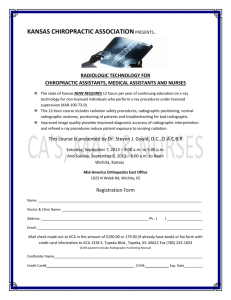
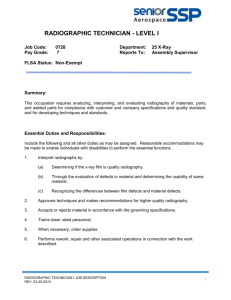
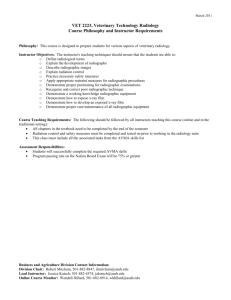
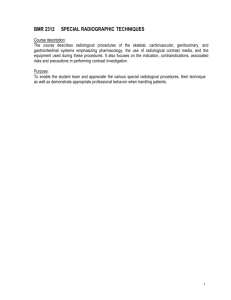
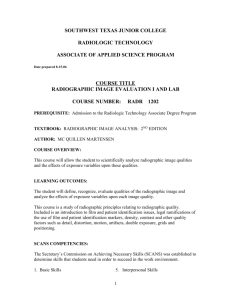
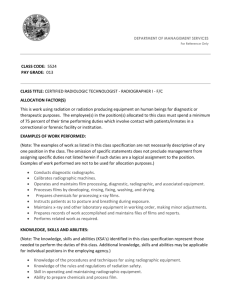
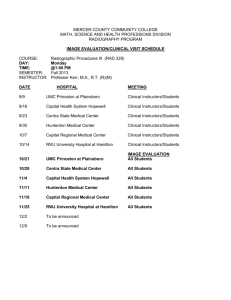
SIMULATION OF THE RADIOGRAPHY FORMATION PROCESS FROM CT PATIENT VOLUME P.Bifulco, M. Cesarelli, E. Verso, M. Roccasalva Firenze, M. Sansone and M. Bracale University of Naples “Federico II”, Electronic Engineering Dept., Bioengineering Unit Via Claudio, 21 - 80125 Naples Italy. Phone: +39 81 7683107 E-mail: bifulco@diesun.die.unina.it Abstract The aim of this work is to develop an algorithm to simulate the radiographic image formation process using volumetric anatomical data of the patient, obtained from 3D diagnostic CT images. Many applications, including radiographic driven surgery, virtual reality in medicine and radiologist teaching and training, may take advantage of such technique. The designed algorithm has been developed to simulate a generic radiographic equipment, whatever oriented respect to the patient. The simulated radiography is obtained considering a discrete number of X-rays paths departing from the focus, passing trough the patient volume and reaching the radiographic plane. To evaluate a generic pixel of the simulated radiography the cumulative absorption along the correspondent X-ray is computed. To estimate X-ray absorption in a generic point of the patient volume, 3D interpolation of CT data has been adopted. The proposed technique is quite similar to those employed in Ray Tracing. A computer designed test volume has been used to assess the reliability of the radiography simulation algorithm as a measuring tool. From the errors analysis emerges that the accuracy achieved by the radiographic simulation algorithm is largely confined within the sampling step of the CT volume. Key words: simulated radiographic projections, ray tracing, virtual reality. 1. INTRODUCTION An algorithm that generates simulated radiographic images using a CT patient volume is here proposed. Many applications may take advantage of generically oriented simulated radiographic projections of a specific patient volume. The method here proposed simulates the functioning of a real radiographic equipment [1]. The simulation algorithm is initialised with the geometrical data of the device to be simulated. The relative position of the device respect to the patient is also specified. The information relative to the patient are provided by a previously recorded CT volume. A virtual radiography is then obtained simulating the radiographic formation process, considering a discrete number of X-rays paths departing from the focus, passing trough the patient volume and reaching the radiographic plane. In this study only CT volumes have been considered to represent the patient because they provide directly volumetric X-ray absorption values. It is also possible to obtain simulated radiographic projections relative to predefined sub-volumes or segmented anatomical structures. This method could constitute a valid support in the field of stereo-tactic or radiographic driven surgery in estimating the 3D relative positioning of internal anatomical structures and surgical tools (e.g. catheters, scalpel, etc.) [2] [3] in combination with a single plane fluoroscopy. Previous studies [4] [5] have utilised simulated radiographic projection of implanted prosthesis structures to dynamically evaluate in vivo their functioning. Another study [6] have analysed the optimal alignment of hip prosthesis during the implanting operation. This technique can be extended to the study of 3D body joint kinematics [7][8][9][10]. Another field of application is the teaching and training of the radiology personnel. This kind of virtual reality technique [11] enables medical staff and trainees to practice and perfect medical procedures without causing discomfort to patients or placing them at risk. These applications require different grades of the simulated images quality. The resolution and the quality of the simulated radiographic images mainly depend on the CT volume resolution. The resolving power of such simulated device is obviously limited by the sampling step of the CT volume, according to the sampling theorem [12]. The radiography simulation algorithm here presented can be regarded as a particular application within the ray-tracing techniques. In fact the radiographic image is obtained evaluating the optical path of the rays that contribute to its formation. The total absorption along the X-ray optical path is computed simulating the real phenomenon of the radiographic image formation. In this work the secondary radiation or scattering effect (raising from the interaction between the X-radiation and the biological tissue) has been not taken into account. This assumption does not constitute a limitation, on the contrary provides the “best” quality for radiogram with respect to the scattering problem. 2. METHOD 2.1 Simulation of the radiographic image formation A CT volume represents the patient’s anatomical structure of interest (patient volume Fig.1). An orthonormal Oxyz reference frame is considered aligned to the axes of the CT volume (Fig. 3). Such reference frame, fixed respect to the patient volume, constitutes the main reference frame. The advantage of using this particular reference frame is that the CT volume planes usually correspond to the anatomical planes: xy represents the horizontal plane, xz represents the coronal (frontal) plane and yz represents the sagittal plane (Fig. 1 and Fig.3). The Fig. 3 represents schematically a generic CT volume and the notation adopted in this work. Figure 1: Schematic representation of the X-ray source, the patient volume and the radiographic plane π respect to the main reference frame Oxyz. Figure 2: Placement of the X-ray source, the patient volume and the radiographic plane π respect to the main reference frame Oxyz. It is also represented the additional reference frame Cunv. The radiographic plane (π) co-ordinates are expressed relatively to the main reference frame. The plane is specified assigning (giving) the co-ordinates of a point C (belonging to the plane) and its orientation in the space. For sake of simplicity, an additional reference frame Cunv fixed on the plane has been considered (Fig.2). The radiographic plane π is fully identified by the point C and the axes u and v. The simulated radiography is obtained on a confined domain, analytically described on the plane π. The radiographic domain is sampled along the axes u and v, respectively with the sampling step ∆u and ∆v (Fig.4). The generic point belonging to the sampling grid on the radiographic plane is identified by P’pq (Fig.4). ∆y v ∆z ∆x P 'p q Rv ∆v Ru n C u ∆u π Figure 3: CT volume, sampling of the patient volume. The three steps of sampling are reported ∆x, ∆y and ∆z. ∆x and ∆y represents the resolution of the CT slice (pixel size), while ∆z is the slice thickness. Figure 4: Sampled domain on the radiographic plane. The additional reference frame Cunv, the sampling steps ∆u and ∆v are reported. The circular shape of the radiographic domain reminds the shape of a fluoroscopic device output. The X-ray source is modelled as a single point F. It constitutes the focus of the simulated radiographic device. For simplicity, the projection of the point F on the radiographic plane π is C. Consequently, the focus F belong to the axis n, normal to the plane π. The distance FC represents the focal distance of the simulated radiographic device. To describe the position of the radiographic plane respect to the main reference frame only the coordinates of the point C and the components of a vector în normal to that plane are needed. For simplicity the additional reference frame (fixed on the radiographic plane) is expressed as a rigid roto-translation of the main reference frame. The orientation of the radiographic plane results from a sequence of simple rotation around the xyz axes. This operation can be expressed by a rotational matrix resulting by a sequence of products of three orthogonal matrices representing the simple rotations around the xyz axes. It is important to choose, even in an arbitrary way, the order of the rotations around the axes. In this way the additional reference frame Cunv results, by construction, ortho-normal. To position the radiographic plane three angles and a vector are used, according to the roto-translation formula [13]. ’ ( ) = t + R ( ) where R = Rz(ϕ)Ry(θ)Rx(ψ) 1 0 0 c ϕ − s ϕ 0 cϑ 0 sϑ R z (ϕ) = sϕ cϕ 0 R y (ϑ) = 0 1 0 R z (ψ) = 0 cψ − sψ 0 sψ cψ 0 − s ϑ 0 cϑ 0 1 where the symbols c and s respectively stay for cosine and sine. This formulation corresponds to perform a first rotation ψ around the x-axis, a second rotation θ around the y-axis and a third rotation ϕ around the z-axis (Fig. 5). In this way the patient volume is considered still and the device moving, of course it is always possible to bring back to the opposite case, inverting the relation: -1 ’ ( ) = R [ ( ) – t] z R z ( ϕ) x R y ( θ) R x ( ψ) y O Figure 5: Simple rotation around the xyz axes. To represent the generic X-ray path relative to a generic point of the sampled radiographic domain, the line connecting F and the generic point P’pq is computed. In this way the X-ray path is considered a straight line: no scattering phenomena have been considered. The algorithm computes X-ray paths starting from the destination points, as in ray tracing methods. The intersection between the line representing the X-ray path and the patient volume determine the segment on which the X-ray absorption takes place. The point of entrance P1 and the point of exit P2 of the X-ray into the patient volume are computed. The segment delimited by those points, on which compute absorption, is sampled with a step ∆ (Fig. 6). Figure 6: X-ray path into the patient volume. P1 and P2 represent respectively the entrance point and the exit point. Sampling of the absorption segment P1-P2 with step ∆. The length of the segment is d’ and the direction of the ray is îh . The total absorption along the segment P1-P2 has to be estimated. As above explained, the segment is sampled with step ∆. To estimate the absorption of a single point internal to the patient volume an algorithm of trilinear interpolation [14] [15] [16] has been adopted. Trilinear interpolation is the process of linearly interpolating points within a box (3D) given values at the vertices of the box. The operation of interpolation is equivalent to convolving the samples with an equivalent reconstruction filter [14]. The entire algorithm results in an estimation of the radiographic image which would be obtained using a radiological device of the same characteristic (e.g. focal distance, domain size, …) equally positioned and oriented respect to the patient. Different kind of X-ray films and/or X-ray detectors can be easily simulated applying simple image postprocessing algorithms. 2.2 Spherical co-ordinates To simply describe relative motion and orientation of the patient respect to the radiographic device a spherical co-ordinates reference system is more immediate and manageable. The radiographic plane may be considered tangent to a spherical surface of ray ρ in a point expressed by two angle α and β. The point C of the radiographic plane corresponds to the contact point with the sphere. The centre of the sphere may be arbitrarily chosen coincident with the centre of the patient volume. The centre of the patient volume is here named M and has co-ordinates (a/2, b/2, c/2) as in figures 3 and 6. Such set-up resembles the practical use of the radiography and simply expresses the relative orientation of the patient. 3 RESULTS AND CONCLUSION 3.1 Assessment of the radiographic simulation method To evaluate the functionality of the radiography simulation algorithm as a measuring tool, a test volume has been designed by computer. The volume containing three non-aligned spherical markers with a diameter of 2 mm (s1, s2, s3) has been built for the purpose (Fig. 7). Its dimensions have been chosen of 60×60×50 mm. The sampling steps of the test volume (∆x, ∆y, ∆z), the sampling steps of the simulated radiographic image (∆u, ∆v) and the sampling step of integration along the X-ray (∆) have been all chosen equal to 1 mm. The focal distance was set to 1m and ρ to 10 cm. The image formation process have been computed following two separate ways: first analytically (control values) and then using the radiography simulation algorithm (estimated values). Afterwards, the two groups of results, obtained independently, have been compared computing the co-ordinate differences on the radiographic plane. Actually only the centres of the markers have been projected analytically on the radiographic plane. These results have been compared with the centroids of the markers projected using the radiography simulation algorithm (Fig. 7 - s1’, s2’, s3’). Figure 7: Assessment of the radiographic simulation method: representation of the test volume and the simulated radiographic projection The spherical co-ordinates reference system, centred in the middle of the test volume, has been utilised for the purpose. To give a statistical characterisation to the test the comparison between the results has been repeated for more than 30 times. Uniformly distributed, random value for ρ, α and β have been used. In the following scatter diagram (Fig. 8) are represented the relative errors of the estimated markers’ coordinates respect to the analytically computed control values. In the centre of the graph, the point with coordinates (0,0) represents the control values. Relatively, the co-ordinates estimated by means of the radiographic simulation algorithm are plotted as crosses. The following table reports the mean value and the standard deviation of the errors' distribution. Difference on u-axis Difference on v-axis Distance Mean [mm] -0.01 0.01 0.14 Standard deviation [mm] 0.10 0.15 0.10 The errors are all contained in the range -0.4, +0.4 mm on both axes. Hence they result to be much smaller than the sampling steps (∆x =∆y = ∆z = ∆u = ∆v = 1mm) used in the simulation of the radiographic image formation. The following graphs report the histograms of the relative frequencies of occurrences for the errors on the u-axis (Fig. 9), the errors on the v-axis (Fig. 10) and the distance between the control values and the estimated co-ordinates (Fig. 11). Figure 8: scatter diagram of errors on co-ordinates (distribution of errors on the radiographic plane) Figure 9: errors on the u-axis. Relative frequencies of occurrences for the differences on the co-ordinates on the u-axis (a gaussian with the same mean and standard deviation is superimposed) Figure 10: errors on the v-axis. Relative Figure 11: distribution of the modulus of the error. frequencies of occurrences for the differences on the Relative frequencies of occurrences (a Rayleigh with co-ordinates on the v-axis (a Gaussian with the same the same characteristics is superimposed) mean and standard deviation is superimposed) coronal view sagittal view Figure 12: Simulated radiographic projections of a selected tract of the lumbar spine Source Visible Human Project CT fresh female. Since the error distributions, on both axes, depend on many factors, they have been hypothesised gaussian. To allow an easy visual comparison, same sized gaussian profiles have been superimposed to the error distributions. Since the error distribution on both axes are almost zero-mean and of similar standard deviation the distribution of the error distances have been hypothesised as a Rayleigh. To assess whether or not the error distributions along the image axes are well approximated by a gaussian, the chi-square test has been performed with a confidence level of 0.05. The hypothesis of gaussian distribution is accepted for the errors on the u-axis but rejected for the errors on the v-axis. In future other interpolation method could be employed to achieve a better estimation of the generic point in the patient volume. Among those are: spline (polynomial) interpolation, sinc and trunked sink interpolation etc. Acknowledgement: The authors wish to thank The Visible Human Project (http://www.nlm.nih.gov/research/visible/) which provides a complete, anatomically detailed, three-dimensional representation of the male and female human body. Transverse CT, MRI and cryosection images of representative male and female body at one millimetre intervals are available. We would like to thank the British Council (British-Italian Collaboration in Research and Higher Education) for generously funding part of the research. Tanks go also to the Italian Ministry of Research and University MURST 40 % . Bibliography [1] E. Verso, Sviluppo di un algoritmo generale per la simulazione di proiezioni radiografiche a partire da volumi 3D. University of Naples “Federico II” Dept. of Electronic Engineering internal report n. T203 [2] S. Lavallèe, P. Cinquin, R. Szeliski, O. Peria, A. Hamadeh, G. Champleboux and J. Troccaz, Building a hybrid patient’s model for augmented reality in surgery: a registration model, Computers in Biology and Medicine March 1995. [3] R. Koppe, E. Klotz, J. Op de Beek, H. Aerts, Digital streotaxy/stereotactic procedures with C-arm based Rotation-Angiography (RA). Proceedings of the International Symposium on Computer System for Image Guided Diagnosis and Therapy, Computer Assisted Radiology CAR ’96, 1996. [4] S. A. Banks, A.Z. Banks, F.F. Cook, W.A. Hodge, Markerless Three Dimensional Measurement of Knee th Kinematics Using Single-plane Fluoroscopy. Proceeding of the 20 Annual Meeting of the American Society of Biomechanics, Atlanta October 17-19, 1996. [5] S. A. Banks, W.A. Hodge, Accurate Measurement of Three-dimensional Knee Replacement Using Single-plane Fluoroscopy, in press IEEE Trans. Biomed. Eng., Vol. 43, No. 6,1996. [6] A.M. DiGioia, D.A. Simon, B. Jaramaz, M. Blackwell, F. Morgan, R.V. O'Toole, B. Colgan, and E. Kischell. HipNav: Pre-operative Planning and Intra-operative Navigational Guidance for Acetabular Implant Placement in Total Hip Replacement Surgery. Computer Assisted Orthopedic Surgery, 1996. [7] P. Bifulco, M. Cesarelli, M. Roccasalva Firenze, E. Verso, M.Sansone and M. Bracale, Estimation of the 3D Positioning of Anatomic Structures from Radiographic Projection and Volume Knowledge, Proceedings of VIII Mediterranean Conference on Medical and Biological Engineering and Computing, Medicon 98 Lemesos Cyprus, June 14-17 ,1998 (this Issue). [8] M. Roccasalva Firenze, Stima dell’orientamento 3D di strutture anatomiche tramite simulazione di proiezioni radiografiche. University of Naples “Federico II” Dept. of Electronic Engineering internal report n. T204 [9] Bifulco, P., Cesarelli, M., Allen, Muggleton, J.M., R., Bracale, M., Automatic Vertebrae Recognition throughout a Videofluoroscopic Sequence for Intervertebral Kinematics Study Time Varying Image Processing and Moving Object Recognition, 4 - Cappellini ed. , Elsevier 1996 [10] P. Bifulco, M. Cesarelli, M.Sansone, R. Allen and M. Bracale. "Fluoroscopic Analysis of Intervertebral Lumbar Motion: a Rigid Model Fitting Technique". World Congress on Medical Physics and Biomedical Engineering, Nice September 14-19, 1997 [11] J.P. Rolland, D.L. Wright, and A. Kancherla Towards a novel augmented reality tool to visualize dynamic 3D anatomy. Proceeding of Medicine meets Virtual Reality, 1997. [12] A.V. Oppenheim, R.W. Schafer, Digital Signal Processing, Prentice Hall International, 1975. [13] L. Sciavicco, B. Siciliano, Robotica Industriale Mc Graw-Hill, 1995. [14] Ingrid Carlbom. Optimal filter design for volume reconstruction and visualization. In IEEE Visualization '93, pp. 54-61, October 1993. [15] Don P. Mitchell and Arun N. Netravali. Reconstruction filters in computer graphics. John Dill, editor, Computer Graphics (SIGGRAPH '88 Proceedings), Vol. 22, pp. 221-228, August 1988. [16] Stephen R. Marschner and Richard J. Lobb. An Evaluation of Reconstruction Filters for Volume Rendering. In IEEE Visualization '94, 1994