Introduction to Radiographic Imaging
advertisement

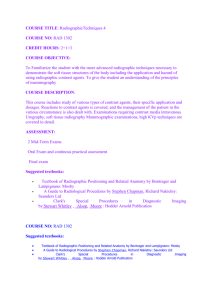
10/20/2011 Introduction to Radiographic Imaging Image Interpretation Objectives » The student will be able to: Correctly review a radiographic study conventional anatomic terminology Correctly name a radiographic view Correctly “hang” a radiographic image List and explain the roentgen signs Know and identify the five radiographic opacities Use Review » Radiograph is picture of x-rays able to penetrate object – literal shadow of object » Differential absorption of x-rays passing through tissues is basis of radiography » Radiograph is a two-dimensional depiction of a three-dimensional object 1 10/20/2011 Principles of interpretation » Review radiographs in appropriate environment (low lighting, quiet) » Be sure to have appropriate views and complete study » “Hang” or display radiographs in a standard manner » Make sure patient positioning and preparation are adequate » Make sure radiographic technique is appropriate » Evaluate entire radiograph systematically Principles of interpretation » Radiographic interpretation need not be mysterious Knowledge of normal radiographic anatomy and possible variants is required! Be systematic Use basic radiographic signs Formulate a differential diagnosis list Conventional Terminology » Use same terminology as in anatomy class » Trunk: cranial, caudal, dorsal, ventral » Head: rostral, caudal, dorsal ventral » Extremity Above carpus and tarsus: cranial, caudal, proximal, distal At and below carpus and tarsus: Front limb: dorsal, palmar, proximal, distal Rear limb: dorsal, plantar, proximal, distal 2 10/20/2011 Conventional Terminology Application Question » “Collimation” refers to restricting the x-ray beam to the confines of the imaging plate. What is one important reason to do this? Radiographic Views » Named according to the direction of the x-ray beam as it penetrates the body part from point-of-entrance to point-of-exit For example, during a ventrodorsal projection of the thorax, the beam enters the ventral aspect of the thorax and leaves the dorsal aspect of the thorax while the patient is in dorsal recumbency 3 10/20/2011 Ventrodorsal (VD) view of thorax X-ray beam Ventrum Dorsum Radiographic Views » Technically, lateral views of abdomen/thorax should be described as “right to left lateral” or “left to right lateral” Convention shortens name: Left lateral – patient in left lateral recumbency Right lateral – patient in right lateral recumbency » Technically, lateral views of extremities should be described as “lateromedial” or “mediolateral” Convention shortens name: Lateral Right lateral view of the abdomen X-ray beam Left lateral aspect R Right lateral aspect 4 10/20/2011 Dorsopalmar (DP) view of carpus From Tech of Vet Rad, 5th ed, Morgan JP, 1993 Radiographic Views » Oblique views are views that are made off angle from the standard lateral and DP/CrCd views Still named by the path of the x-ray beam Technically should include angle of obliquity (dorsal 60º lateral-palmaromedial oblique) Not needed for standardized views However, degree of obliquity does change appearance Dorsolateral-plantaromedial (DLPM) oblique view of tarsus From Tech of Vet Rad, 5th ed, Morgan JP, 1993 5 10/20/2011 Why oblique views? » Generally, abnormalities (fractures, bony reactions, etc) are easier to see if the x-ray beam strikes them tangentially » Abnormalities are much more difficult to see if the x-ray beam strikes them head-on (en face) » Nearly obligatory for complex structures (equine carpus and tarsus, skull) En face versus tangential En face Tangential Application Question » What is wrong with this radiograph? 6 10/20/2011 Radiographic Image » Through and through concept For a given view (for example, craniocaudal versus caudocranial) it generally does not matter which way the beam enters and leaves the object – image will appear the same Some exception for organ sag and gas distribution seen in thorax and abdomen Radiographic image Displaying or “hanging” radiographs for interpretation » By convention, images are always hung on the view box or displayed on a monitor in the same manner Assists in developing picture of normal anatomy 7 10/20/2011 Displaying or “hanging” radiographs for interpretation » Ventrodorsal (VD)/Dorsoventral (DV) view of trunk Cranial portion of image at top of viewing screen Patient’s left positioned on viewer’s right Ventrodorsal (VD)/ Dorsoventral (DV) View Patient’s head (cranial) Patient’s left Patient’s right Patient’s rear (caudal) Displaying or “hanging” radiographs for interpretation » Lateral view of trunk Dorsal portion of image at top of viewing screen Cranial portion of image positioned on viewer’s left 8 10/20/2011 Lateral View Patient’s dorsum Patient’s Head (cranial) Displaying or “hanging” radiographs for interpretation » Craniocaudal (CrCd)/Caudocranial (CdCr), Dorsopalmar (DP)/Palmarodorsal (PD), Dorsoplantar (DP)/Plantarodorsal (PD) of extremities Proximal portion of image at top of viewing screen Viewer’s discretion how to place medial and lateral aspects of image Consider hanging as if looking at the patient OR place lateral aspect of the limb on the viewer’s left Dorsopalmar View Proximal L A T E R A L L A T E R A L Medial Left Right Distal 9 10/20/2011 Dorsopalmar View Proximal L A T E R A L L A T E R A L Left Right Distal Displaying or “hanging” radiographs for interpretation » Lateromedial (lateral)/mediolateral (lateral) view of extremities Proximal portion of image at top of viewing screen Cranial (or dorsal) portion of image positioned on viewer’s left Lateromedial View Proximal Caudal Cranial Plantar Dorsal Distal 10 10/20/2011 Lateromedial View Proximal R Cranial Caudal Distal Application Question » Why can’t we tell where the lumen of the heart chambers are on a radiograph? Displaying or “hanging” radiographs for interpretation » Important concept: You cannot determine right from left without anatomic or artificial markers Must incorporate positioning markers with images convention, the positioning markers should be placed at the lateral aspect or the cranial/dorsal aspect of an extremity By 11 10/20/2011 Which Limb? Radiographic Image REMEMBER: » Two-dimensional shadow of a threedimensional object Need at least two orthogonal views to portray object faithfully Necessity of two views 12 10/20/2011 Necessity of two views Roentgen Signs » Identify radiographic abnormalities (Roentgen signs) Opacity Size Shape Number Location/position/alignment Margination Function Radiographic Opacities » Five basic radiographic opacities Air (gas) opacity – black Fat opacity – dark gray Fluid/Soft tissue opacity – light gray Bone Fluid: water, blood, urine, etc Soft tissue: muscle, organ Bone opacity – gray white Metal opacity – white Air Fat Fluid Metal 13 10/20/2011 Radiographic Opacities Bone Air Metal Fat Fluid/Soft tissue Roentgen Signs example Roentgen Signs example » Opacity – soft tissue 14 10/20/2011 Roentgen Signs example » Size – 13 cm long x 8 cm high Roentgen Signs example » Shape – ovoid Roentgen Signs example » Number – one 15 10/20/2011 Roentgen Signs example » Location – cranioventral abdomen near tail of spleen Roentgen Signs example » Margination – irregular or lobulated Roentgen Signs example » One ovoid, lobulated, 13 x 8 cm, soft tissue mass in the cranioventral abdomen 16 10/20/2011 Goal of Imaging » Create an image that will faithfully represent what is going on in the area of the patient being imaged while limiting exposure to the patient and those handling the patient Application Question » Which view of the tarsus is being made? A. Craniocaudal B. Caudocranial C. Dorsoplantar D. Plantarodorsal Summary » Radiographic views named by path of x-rays using conventional terminology » Always display or “hang” radiographs in a standard manner » Evaluate radiographs using Roentgen signs to describe findings » There are five basic radiographic opacities 17