Bedside handover process
advertisement

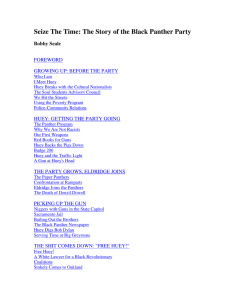
STANDARD WORK Bed Side Handover process from shift to shift Operation: Equipment; Parts; Tools; Materials Related Documents; Forms # • • • • COW (computer on wheels) Green/Red file Ward Procedural Charge File Takeover sheet • WI-NUR-GEN-006 Patient Handover WORK SEQUENCE SW No.: SW-NUR-GEN-001 SW Rev: 1 Effective: 11/04/11 DD/MM/YY STANDARD/SCRIPT Time/ Duration (Specifications, Quality, Safety) 1 PN pushes a COW and arrives at the designated bed with team (PNs, EN/HCA) 2 PN and team taking over shift to approach patient at bedside 1. Greet patient, introduce self and team. Hand over using a low tone of voice that is loud enough for your team to hear but not within earshot of neighbouring patients (this includes anyone who is not supposed to hear). If necessary, move out of the cubicle. 100% compliance of the Script:”Good morning / afternoon / evening Mdm/Mr/Ms XXX, I am Staff Nurse NAME. This is my team. We will be taking care of you during this shift.” 2. Assess for pain Script: “Are you experiencing any pain now? If yes, “On a scale of 0-10, when 0 is no pain and 10 is worst pain. Are you able to rate the current pain you are experiencing?” Observe for sign of distress if unable to verbalize 3. Assess for bowel movement. Script:” Have you pass motion today?” 4. Ask patient if he/she has taken diet, or has sleep well in accordance to shift. 5. Check invasive lines (if any). Any abnormal signs and symptoms of phlebitis, bleeding, loose connections, dislodgements. Script: ND-AM: “Did you sleep well? AM-PM: “Did you eat your lunch?” PM-ND: “Did you eat your dinner?” Exclude patients who are unable to take orally e.g. patient on NBM or NGT Site dated. Dressing clean. 6. Verify infusion - infusion fluid, route and rate (if any). Tally with order in EIMR 7. Check environment- any medication left on the locker, Wearable effects such as ring; bangles and chain on patients not too tight i.e. with two finger spacing which dentures, hearing aids or personal effects present. do not impede circulation. SW Template Rev.B- 20090319 This template is created by TTSH-HRD. For information, please contact Koh Huey Bing: koh_huey_bing@ttsh.com.sg at ext. 8629 or Reandy Yang: reandy_yang_yc@ttsh.com.sg, ext 1894 8. Verify and update headboard accurately. Name- to write surname/family name with initials. Name Discipline Language/dialect Diet Denture Hearing Aid Functional Status Oral Hygiene PU Care Bundle 9. Reinforce on fall precaution (if applicable) and to emphasize on use of call bell for assistance. 3 Pink headboard and Pink wrist tag for patient on fall risk. PNs to open 4 windows simultaneously to view clinical information together. 1. SmartSense - Vital signs trending, Pain score, Bowel Deranged /abnormal reading is reported. - Drainage (where applicable) - Weight (where applicable) - POD (where applicable) 2. EIMR - Open ‘View all Med’ page to view the active medication list. - Ensure medications are served timely. Timing as reflected in the Inpatient Med Admin page in EIMR. - Valid reasons are available for omission of medicine. Indicate Timing - Non-omnicell medications are available. - Odd timing medications to be served at during shift are noted. Recommendation: For odd timing medications, can use flagging board as reminder. 3. Aurora - Type of lab / radiology investigations ordered - Status of investigations / appointments Deranged /abnormal result is reported. - Results 4. EMOS - Verified types of diet ordered. Tally with Nursing Kardex and headboard. SW Template Rev.B- 20090319 This template is created by TTSH-HRD. For information, please contact Koh Huey Bing: koh_huey_bing@ttsh.com.sg at ext. 8629 or Reandy Yang: reandy_yang_yc@ttsh.com.sg, ext 1894 4 PNs to go through the documents in the green/red folder together. To communicate if any issues arise. Team to verify records and monitoring charts are updated. - Treatment sheet (include updates from continuation sheet, refer to clinical pathway if applicable) - Nursing Kardex - Monitoring Charts (E.g. Fluid regime, Diabetic, CLC, Intake/ Output, Chest Tube, Restrainer, Suctioning, Neurovascular, Peak Flow, Suicide Caution, Fall prevention, oral hygiene, PU Bundle Form Fits chart, Postural BP). 5 AN/HCA clarify with PN if any queries. AN / HCA check in blue folder: - Ward procedural charge form Ensure all procedures done and consumable are charge accordingly PN hands over patient information based on the PCR, Clinical pathway, PFE, discharge planning, mWheFRA score, and communication chart, where applicable. Use structured takeover sheet e.g. Trendcare patient report for note taking. - Not to update on the spot. - Any new changes updated by PNs after handing over to be communicated before going off shift. 6 PN taking over shift to clarify any doubts Move on to patient at next bed when ready Repeat step 2-6 till PN and team reach the last patient assigned Created by: Lum Yuat Soon / Tan Tzuu Ling Department: Nursing Service Ext: 3008 7 Approved by: Validated with: Kwek Puay Ee Director, Nursing Nursing Standards Committee SW Template Rev.B- 20090319 This template is created by TTSH-HRD. For information, please contact Koh Huey Bing: koh_huey_bing@ttsh.com.sg at ext. 8629 or Reandy Yang: reandy_yang_yc@ttsh.com.sg, ext 1894