Noelle Johnstone, MD
advertisement

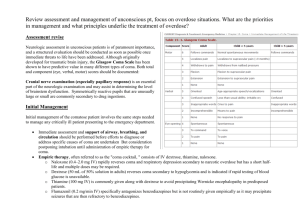
Altered Mental Status Noelle Johnstone, MD General Pediatrics Dec. 22, 2009 YouTube: • “David After Dentist” Altered Mental Status Noelle Johnstone, MD General Pediatrics Dec. 22, 2009 Overview • Altered Mental Status – Mental Status Exam • Topic Review with a NEJM Case • Coma in Pediatrics • Ethanol intoxication in Pediatrics Altered Mental Status in Pediatrics Subtle Cognitive Difficulties shortened attention span impaired memory perceptual deficits personality changes agitation disorientation Florid Delirium … Coma LETHARGY … obtundation … STUPOR YouTube: • “SESAME STREET NOW!!” Mental Status Examination • • • • • • • • Appearance, attitude, and behavior/activity Mood and affect Speech Thought process Thought content Perception Insight and judgment Cognition: Sensorium and intelligence Blue Team Case • TC, 6 yo previously healthy female (12/1/09) • CC: Behavioral changes x 10 days, “vacillating … euphoria, anger… at times, … extremely sedated” • ROS: – Difficulty with word‐finding and comprehension – Urinary incontinence 3 times this week – 15 pounds weight loss in recent months – Regression in reading skills Blue Team Case • TC, 6 yo previously healthy female (12/1/09) • CC: Behavioral changes x 10 days, “vacillating … euphoria, anger… at times, … extremely sedated” • PE: “The patient appears dazed and confused. … is neither effectively communicating thoughts, only intermittently following commands, at times appearing euphoric, and then at other times, appearing quite sedated and, finally, having intermittent flash periods of anger and thrashing about the room.” Altered Mental Status: AEIOU TIPS • • • • • Alcohol Encephalopathy / Electrolytes Insulin/ Intussusception Overdose Uremia • • • • Trauma Infection Psychiatric condition Seizure Some definitions… • Psychosis • Toxic‐Metabolic Encephalopathy • Delirium "Mayeh mambo dogface to the banana patch?" Psychosis • Disturbance in perception of reality: – Hallucinations, – Delusions, or – Thought disorganization (loose associations, nonsensical speech, bizarre behavior) • Risk for agitation, aggression, impulsivity • Disorders: – Schizophrenia, Bipolar mania, MD with psychotic features, – Delirium, Brief Psychotic disorder, – Substance‐induced psychotic disorder, – Psychosis secondary to a medical condition Acute Toxic‐Metabolic Encephalopathy (TME) • Global cerebral dysfunction → altered consciousness, behavior changes, seizures • Not due to primary structural brain disease (tumor or hemorrhage) or infection • Interference with the function of the ascending reticular activating system (RAS) Oski's Pediatrics. 2006. Delirium from L. deliriare "be crazy, rave" • Reduced ability to focus/sustain/shift attention • Hyperactivity and diminished sleep • Confusion, excitement, hallucinations, irritability American Psychiatric Association, Diagnostic and Statistical Manual, 4th ed, APA Press, Washington, DC 1994. Adams and Ropper. Delirium and other acute confusional states. Principles of Neurology, 6th ed, McGraw­Hill, NY 1997. Altered Mental Status: History • Obtain a complete description of the progression of mental status alteration – Onset, progression, recurrence • Family History: – impaired responsiveness, CVA, stroke, cyanotic heart disease, sickle cell disease, DM, hypoglycemia, or IEOM • PMH: – Trauma, recent illness, intoxication, CO exposure, lead, heat exposure, psychiatric illness Altered Mental Status: Physical • ABC’s • Respiratory patterns: – HYPERventilation • • • • Compensation for metabolic acidosis Primary respiratory alkalosis Central hyperventilation – midbrain dysfunction Compensation for hypoxia – HYPOventilation • Compensation for metabolic alkalosis • Respiratory acidosis – Cheyne‐Stokes respirations Altered Mental Status: Physical • Decorticate Posturing – Arms FLEXED and adducted, Legs EXTENDED – Corticospinal tract lesion, within or near cerebral hemispheres UpToDate, Evaluation of Stupor and Coma in Children, Fig. 2 Altered Mental Status: Physical • Decerebrate Posturing – Arms EXTENDED, internally rotated, Legs EXTENDED – Brainstem involvement – Metabolic abnormality UpToDate, Evaluation of Stupor and Coma in Children, Fig. 2 Altered Mental Status: Pupils • Pinpoint (1‐2 mm) and Fixed • Pontine lesion • Opioid intoxication • Small (2‐3 mm) and Reactive • Medullary lesion • Metabolic abnormality • Dilated and Fixed – Bilateral: diffuse brain damage, HIE – Unilateral: seizures, herniation, CN III lesion Gray’s Anatomy. Toxidromes: Miosis • Opioid – CNS depression, coma • Sedative‐hypnotic – CNS depression, confusion, stupor, coma • Cholinergic – Confusion, coma Toxidromes: Mydriasis • Sympathomimetic – Hyperalert, agitation, hallucinations, paranoia • Anticholinergic – Hypervigilance, agitation, hallucinations, delirium with mumbling speech, coma • Hallucinogenic – Perceptual distortions, depersonalization, synesthesia, agitation • Serotonin Syndrome – Confusion, agitation, coma • Tricyclic Antidepressants – Confusion, agitation, coma Altered Mental Status: Eye Movements • Oculocephalic (doll’s eye) reflex • Oculovestibular (caloric) reflex YouTube: • “Cold calorics in an awake, alert subject” Altered Mental Status: Eye Movements • Nerve VI palsy – Increased ICP – Meningeal irritation – Pontine lesion • Nerve III palsy (“down ‘n out”) – Herniation – Midbrain lesions – “setting sun” CN III – down n’ out CMAJ Oct. 16, 2006; 175(8) p. 878. CMAJ Oct. 16, 2006; 175(8) p. 878. Increased ICP • Early: – Headache, persistent vomiting – Flat affect, poor feeding, lethargy • …Next: – Papilledema, macrocephaly, split sutures, bulging fontanel – Bradycardia • Late: – HTN, bradycardia, respiratory depression (Cushing’s triad) – Hemiparesis, hyperreflexia, and hypertonia – Obtundation/ coma ©2009 UpToDate® Papilledema ©2009 UpToDate® And now… A True Story… NEJM Case 38‐2003: A 12‐Year‐Old Girl with _______ • Previously healthy 12‐year‐old girl presents with fever, vomiting • HPI: She had been well until one week earlier, when a cough, sore throat, and rhinorrhea developed… NEJM Case 38‐2003: A 12‐Year‐Old Girl with _______ • Evening before admission, temp was 39.4°C • On the day of admission she began to vomit and was taken to the emergency department • Vitals: T 39.2°C, HR 121, BP 135/75, Sp02 98% • She was alert, fully oriented, able to walk, and able to talk coherently NEJM Case 38‐2003: A 12‐Year‐Old Girl with _______ • 75 minutes after arrival, flexion of her elbows and extension of her knees occurred • The patient began to stare straight ahead, became unresponsive to verbal stimulation, and was incontinent of urine • Painful stimulation provoked increased flexural posturing and moaning NEJM Case 38‐2003: A 12‐Year‐Old Girl with _______ • 12 yo girl with fever, emesis, and abrupt onset of unresponsiveness with decorticate posturing • What next? Altered Mental Status: AEIOU TIPS • • • • • Alcohol Encephalopathy / Electrolytes Insulin/ Intussusception Overdose Uremia • • • • Trauma Infection Psychiatric condition Seizure Altered Mental Status: Etiologic Considerations • Infection: – Meningitis, Encephalitis, Intracranial abscess, Subdural empyema • Seizures • Vascular conditions: – Subarachnoid hemorrhage, Hypertensive encephalopathy, CVA • Endocrine/Metabolic: – Hypoglycemia, DKA, Hypo‐/Hypernatremia, Renal failure, Reye’s encephalopathy, Addison crisis, IEOM • Neoplasms • Trauma: – Cerebral concussion, Subdural/Epidural hematoma, Drowning, Heat Stroke • Intoxication: – Sedative‐hypnotics, Narcotics, EtOH, Salicylates, CO, Lead • Psychiatric conditions NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • 75 minutes after the patient's arrival, flexion of her elbows and extension of her knees occurred • The patient began to stare straight ahead, became unresponsive to verbal stimulation, and was incontinent of urine • Painful stimulation provoked increased flexural posturing and moaning NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • 75 minutes after the patient's arrival, flexion of her elbows and extension of her knees occurred • The patient began to stare straight ahead, became unresponsive to verbal stimulation, and was incontinent of urine • Painful stimulation provoked increased flexural posturing and moaning Glasgow Coma Scale “E – V – M. 4 – 5 – 6!” • E4 – “Spontaneous” E3 – To voice E2 – To pain E1 – Ø EYES • V5 – “Spontaneous”/smiles, interacts V4 – Disoriented, Confused / cries, irritable but consolable V3 – Inappropriate Words / cries with pain, aware of environment V2 – Sounds / moans with pain or inconsolable crying V1 – Ø VERBAL • M6 – “Spontaneous” M5 – Withdraws to touch (localizes) M4 – Withdraws to pain (withdraws) M3 – Decorticate to pain (flexion) M2 – Decerebrate to pain (extension) M1 – Ø MOTOR Performance of the pediatric Glasgow coma scale in children with blunt head trauma. Acad Emerg Med 2005; 12:814. NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • Interventions: – A liter of NS was infused – IV lorazepam (4 mg total) ® relaxation of the posture, but the patient remained unresponsive – Phenobarbital 750 mg IV – RSI with thiopental, and succinylcholine; O2 sat 99 – 100% with BMV – Cultures drawn, vanco 1 g + ceftriaxone 2 g IV Hematologic Laboratory Data Hematologic Laboratory Data Warren H et al. N Engl J Med 2003;349:2341­2349 Warren et al. 349 (24): 2341­9, Table 1 December 11, 2003 NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • Transportation by helicopter was arranged • Both pupils 3 mm, with sluggish reactivity • About 15 minutes into the flight, left pupil was dilated to 7 mm, right pupil to 5 mm, both reacted sluggishly to light • Pulse rose to > 200, with an increase in BP • Twenty‐four minutes after the flight had begun, both pupils became fully dilated and unreactive to light NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • PICU examination: – Warm and well‐perfused – Pink, frothy secretions oozed from the ETT – No response to noxious stimuli – Pupils were 7 mm in diameter and fixed – No corneal reflexes, no gag reflex – No spontaneous movement of the legs or arms – ¯muscle tone – Reflexes and the plantar responses were absent NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • Vancomycin, ceftriaxone, TMP‐SMX, acyclovir, pentobarbital, thiopental, & mannitol • CT/ CT angiogram: – diffuse cerebral and cerebellar edema – tonsillar herniation, and – decreased arterial flow in the higher‐order branches of the circle of Willis CT Angiogram Showing Flow within the Proximal Intracerebral Arteries but Little Flow Distal to the Major Branches. Warren et al. 349 (24): 2341­9, Figure 1 December 11, 2003 NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • 3:00 a.m., EVD inserted into the R frontal lobe; opening pressure was >35 cm of water • Drain clamped; brain began to extrude through the drain, → ICP bolt • Hypotension developed → pressors • Neuro exam revealed loss of brain‐stem function • 8:00 a.m., agonal cardiac rhythm occurred, persisted • Several purpuric lesions, each <1 cm, found on the ventral aspect of the R forearm Cutaneous Lesions Warren et al. 349 (24): 2341­9, Figure 5 December 11, 2003 NEJM Case 38‐2003: A 12‐Year‐Old Girl with Fever and Coma • 9:00 a.m., the patient was extubated • Post‐mortem examination of CSF revealed gram‐negative intra‐ and extracellular diplococci, c/w N. meningitidis • Cultures of CSF, brain tissue, and blood obtained at autopsy were all sterile • BCx obtained at the referring hospital before any antibiotics had been given were sterile AMS: Diagnostic Work‐Up • • • • • Glucose, Electrolytes LFTs, ammonia, BUN/Cr CBC with differential Urine / Blood Toxicology, Lead +/‐ ABG, cultures, LP, CT/MRI • Empiric oxygen, glucose, naloxone • Suspected metabolic abnormalities: urine porphyrins, ketone bodies, plasma free fatty acids, carnitine, CK, lactate, pyruvate, serum amino acids, and urine organic acids Initial treatment for hypoglycemia • 10% Dextrose 2.5 mL/kg IV (0.25 grams/kg) • 25% Dextrose 1 – 2 ml/kg IV (0.5 – 1.0 grams/kg) • Glucagon 0.03 mg/kg IM or Sub‐Q (max 1 mg) Rapid treatment for opioid overdose • Naloxone 0.1 mg/kg IV, repeat PRN (0.4 – 2 mg) Rapid treatment for benzo overdose • Flumazenil 0.01 mg/kg, repeat PRN (max 0.2 mg/dose, max cumulative dose 1 mg) Pediatric Coma from Gk. koma “deep sleep” • Coma = "unarousable unresponsiveness” • Nontraumatic: 30 per 100,000 children per year • Traumatic: 140 per 100,000 children per year • Versus: stupor, lethargy, obtundation – Preserve some arousal or awareness Roger’s Textbook of Pediatric Intensive Care, 4 th edition. Nontraumatic Coma in Pediatrics • Prospective, population‐based study of nontraumatic coma in 278 children (UK) • Incidence: – 30.8 per 100 000 children <16 per year – 160 per 100 000 in the first year of life What do you think was the most common etiology? Arch Dis Child 2001 Mar;84(3):193­9. Nontraumatic Coma in Pediatrics • Infection was most common etiology (38%) – Neisseria meningitidis most common (47%) • 2nd most common cause overall? – 10% overall – But the most common cause in adolescents (35%) • Exogenous toxin (accidental + deliberate) Arch Dis Child 2001 Mar;84(3):193­9. Nontraumatic Coma in Pediatrics • Mortality ranged from – 84% (drowning) – 3.4% (intoxication, accidental and intentional) Arch Dis Child 2001 Mar;84(3):193­9. Ethanol Overdose in Pediatrics • 11,000 ethanol exposures in children < 6 years reported to poison control centers / year • 85 ___% due to Ethanol‐containing products other than alcoholic beverages UK NEWS PRISONERS GET DRUNK ON HAND GEL The prisoners had been mixing it with water Friday September 25,2009 By Mark Reynolds Alcoholic hand gel meant to combat swine flu has been removed from a jail after prisoners got drunk on it and started a fight. Instead of rubbing it into their hands, … had been mixing it with water and turning it into hooch. Ethanol Intoxication •ABC’s, glucose • • • • • • 20‐50 mg/dl 50‐100 mg/dl 100‐150 mg/dl 150‐250 mg/dl 300 mg/dl 400 mg/dl • Clearance: ©2009 UpToDate® Diminished fine motor coordination Impaired judgment; impaired coordination Difficulty with gait and balance Lethargy; difficulty sitting upright Coma in the non‐habituated drinker Respiratory depression 10 to 20 mg/dL per hour (Faster in chronic users) THE END… MERRY EVERYTHING! Love, Noelle, Reed & Cole