Intake Wellness Form
advertisement

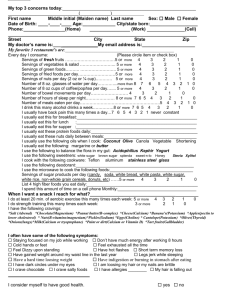
Name: _________________________________________________ Date: _____________ NOTE: This data is used for stress reduction only. Every day I consume: Please circle item Servings of fresh fruits ……………………………….5 or more 4 3 2 1 0 Servings of vegetables & salad …………………….. 5 or more 4 3 2 1 0 Servings of green foods………. …………………….. 5 or more 4 3 2 1 0 Servings of fried foods per day……………………….5 or more 4 3 2 1 0 Servings of nuts per day (2 oz or ¼ cup)……………5 or more 4 3 2 1 0 Number of bowel movements per day……………………………...4 3 2 1 0 Number of hours of sleep per night………………… 8 or more 7 6 5 4 3 2 1 0 Number of meals eaten per day…………………………………………………5 4 3 2 1 0 I usually have back pain this many times a day…………….7 6 5 4 3 2 1 never constant I usually eat this for breakfast:____________________________________________________ I usually eat this for lunch :____________________________________________________ I usually eat this for supper :____________________________________________________ I usually eat these protein foods daily:______________________________________________ I usually eat these nuts daily between meals:________________________________________ I usually use the following oils when I cook: Coconut Olive Canola Vegetable Shortening I usually eat the following: margarine or butter I use the following to balance the flora in my gut: Acidophilus Kephir Yogurt I use the following sweeteners: white sugar brown sugar splenda sweet-n-lo Honey Stevia Xylitol I cook with the following cookware: Teflon aluminum stainless steel glass I use the following deodorant:_______________________________________________________ I use the microwave to cook the following foods:________________________________________ List 4 high fiber foods you eat daily:__________________________________________________ I spend this amount of time on a cell phone monthly:_____________________________________ When I want a snack I reach for what?____________________________________________ I have the following cravings: Please circle item *Salt (Adrenal) *Chocolate(Magnesium) *Peanut butter(B-complex) *Cheese(Calcium) *Banana’s(Potassium) *Apples (pectin to lower cholesterol) *Nuts(B-vitamins/magnesium) *Pickles(Sodium) *Eggs(Choline) *Milk(Calcium or tryoptophane) *Cantelope(Potassium) *Olives(Thyroid) *Onions(lungs) *Tart fruits(Gallbladder) *Paint or dirt(Calcium or Vitamin D) I often have some of the following symptoms: Please check boxes that apply. Staying focused on my job while working Cold hands or feet Don’t have much energy after working 8 hours Feel exhausted all the time Feel Dizzy upon standing Legs jerk while sleeping My hair is falling out Short term memory loss Have a hard time loosing weight Have indigestion or burning in stomach after eating I have dark circles under my eyes I am loosing my hair or my nails are brittle I crave salty foods Have hot flashes I crave chocolate Have gained weight around my waist line in the last year I have allergies (list) ____________________________________________________________________ I consider myself to have good health. yes no I am this ready to make lifestyle changes to become healthier: Not at all I plan to make changes in next 6 months I plan to make changes in next 3 months I plan to make changes in next 30 days Name: _________________________________________________ Date: _____________ In the past two weeks, I have felt: Down, depressed, or hopeless Good Little interest or pleasure in doing things Great I have back pain: no yes, Explain: ___________________________________________ ____________________________________________________________________________ I am coping with my stress level: Very well Well Can’t cope anymore Some trouble Often trouble coping Need help I have had the health conditions I checked below: Heart attack High cholesterol Bypass surgery Stroke Asthma Heart failure High blood pressure Cancer Chronic pain_______(where) Lung disease Arthritis Depression Frequent headaches Diabetes: Type 1 or Type 2 (Age at onset ) I use insulin ___yes ___no I have a brother, sister or parent with diabetes yes no I gave birth to a baby weighing more than 9 #’s yes no Other major medical problems:_________ _________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ Tobacco Use: Never Quit years ago Type of tobacco used __ Current user: Cig. packs Cigar Pipe Chew. Packs per day ____# years____ Other In the past four weeks I have experienced a persistent cough, chest tightness or heaviness, wheezing, extreme fatigue and/or acute shortness of breath. Please circle which symptom(s). Never 2 times/week Daily Continually In past four weeks I have been awakened at night by cough, chest tightness or heaviness, wheezing, and/or shortness of breath. Please circle which symptom(s). Never under 4 times/month 1-2 times/week 3 times or more/week Taking care of me I do the following things to help manage my stress:__________________________________________ _______________________________________________________________________________________ I understand that Kari Uselman, Ph.D., biofeedback practitioner, non-medical doctor, is providing biofeedback and stress reduction. I agree that I am receiving suggestions to improve my health. It is my choice and responsibility to improve my health. These are only suggestions. ___________________________________ Signature ______ _________________________ Date