I regularly take this number of prescription medicines: (please circle)
advertisement
")
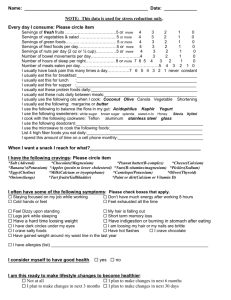
My top 3 concerns today:_____________________________________________________ ____________________________(____________) First name Middle initial (Maiden name) Last name Sex: Male Female Date of Birth: ____-____-____ Age:_____________ City/state born:___________________ Phone:______________ _(Home) ________________ (Work) (Cell) ___________________________________________________________________________ Street City State Zip My doctor’s name is:___ ______________My email address is:_____________________ My favorite 3 restaurant’s are:________________________________________________ Every day I consume: (Please circle item or check box) Servings of fresh fruits ………………………………5 or more 4 3 2 1 0 Servings of vegetables & salad …………………….. 5 or more 4 3 2 1 0 Servings of green foods………. …………………….. 5 or more 4 3 2 1 0 Servings of fried foods per day………………………5 or more 4 3 2 1 0 Servings of nuts per day (2 oz or ¼ cup)………… 5 or more 4 3 2 1 0 Number of 8 oz. glasses of water per day…………...more than 8 7 6 5 4 3 2 1 0 Number of 8 oz cups of coffee/pop/tea per day….... 5 or more 4 3 2 1 0 Number of bowel movements per day……………………… 4 3 2 1 0 Number of hours of sleep per night………………… 8 or more 7 6 5 4 3 2 1 0 Number of meals eaten per day………………………………………………….5 4 3 2 1 0 I drink this many alcohol drinks a week……………8 or more 7 6 5 4 3 2 1 0 I usually have back pain this many times a day…7 6 5 4 3 2 1 never constant I usually eat this for breakfast:____________________________________________________ I usually eat this for lunch :____________________________________________________ I usually eat this for supper :____________________________________________________ I usually eat these protein foods daily:______________________________________________ I usually eat these nuts daily between meals:________________________________________ I usually use the following oils when I cook: Coconut Olive Canola Vegetable Shortening I usually eat the following: margarine or butter I use the following to balance the flora in my gut: Acidophillus Kephir Yogurt I use the following sweetners: white sugar brown sugar splenda sweet-n-lo Honey Stevia Xylitol I cook with the following cookware: Teflon aluminum stainless steel glass I use the following deodorant:___________________________________________________ I use the microwave to cook the following foods:____________________________________ Servings of sugar products per day (candy, soda, white bread, white pasta, white sugar, white rice, non-whole grain cereals, donuts, etc) ……5 or more 4 3 2 1 0 List 4 high fiber foods you eat daily:________________________________________________ I spend this amount of time on a cell phone Monthly:__________________________________ When I want a snack I reach for what?__________________________________ I do at least 20 min. of aerobic exercise this many times each week: 5 or more I do strength training this many times each week: 3 or more I have the following cravings: 4 3 2 2 1 1 0 0 *Salt (Adrenal) *Chocolate(Magnesium) *Peanut butter(B-complex) *Cheese(Calcium) *Banana’s(Potassium) *Apples(pectin to lower cholesterol) * Nuts(B-vitamins/magnesium)*Pickles(Sodium) *Eggs(Choline) * Cantelope(Potassium) *Olives(Thyroid) *Onions(lungs)*Milk(Calcium or tryoptophane) *Paint or dirt(Calcium or Vitamin D) *Tart fruits(Gallbladder) I often have some of the following symptoms: Staying focused on my job while working Don’t have much energy after working 8 hours Cold hands or feet Feel exhausted all the time Feel Dizzy upon standing Have hot flashes Short term memory loss Have gained weight around my waist line in the last year Legs jerk while sleeping Have a hard time loosing weight Have indigestion or burning in stomach after eating I have dark circles under my eyes I crave chocolate I crave salty foods I am loosing my hair or my nails are brittle I have allergies ________ My hair is falling out I consider myself to have good health. yes no I am this ready to make lifestyle changes to become healthier: Not at all I Plan to make changes in next 6 months I Plan to make changes in next 30 days Already changing - less than 6 months Already changing - longer than 6 months In the past two weeks, I have felt Down, depressed, or hopeless Little interest or pleasure in doing things Good Great ________ __________________________ I am coping with my stress level: Very well Well Some trouble Often trouble coping Can’t cope anymore Need help On a scale of 1 to 10 with 10 being the highest, I would rate my stress as a:____________ ___________________________________ I have had the health conditions I checked below. Heart attack High cholesterol Bypass surgery Stroke Asthma Heart failure High blood pressure Cancer Chronic pain_______(where) Lung disease Arthritis Depression Frequent headaches Diabetes: Type 1 or Type 2 (Age at onset ) I use insulin yes no I have a brother, sister or parent with diabetes yes no I gave birth to a baby weighing more than 9 #’s yes no Surgeries (date):_________________________ _ Other major medical problems:_________ Number organs removed:____ Major infections in your lifetime:___ Major toxic exposures in your lifetime:______ Major traumas in your life time:_______ ______ Number of amalgam fillings in my teeth:______ Number of steroid type drugs or street drugs used in the last year: _______________________ Number of unresolved mental factors:_________ Number of kilos overweight as seen by you :__ Tobacco Use Never Quit years ago Type of tobacco used Current user: Cig. packs Cigar Pipe Chew. Packs per day ____# years__ ___________________________________ Medicine I regularly take this number of prescription medicines: (please circle) 0 1-2 3-5 more than 5 My prescription medications are:_________________________________________________ I regularly take these over-the-counter drugs, herbs, vitamins ________________ _________________________________________________________________ ___________________________________ ___________________________________ Other In the past four weeks I have experienced a persistent cough, chest tightness or heaviness, wheezing, extreme fatigue and/or acute shortness of breath(Please circle which symptom) Never 2 times/week Daily Continually In past four weeks I have been awakened at night by cough, chest tightness or heaviness, wheezing, and/or shortness of breath(Please circle which symptom) Never under 4 times/month 1-2 times/week 3 times or more/week Taking care of me I do the following things to help manage my stress:__________________________________________ ___________________________________________________________________________________ I understand that Kari Uselman, Ph.D., biofeedback practitioner, non-medical doctor, is providing biofeedback and stress reduction. I agree that I am receiving suggestions to improve my health. It is my choice and responsibility to improve my health. These are only suggestions. ___________________________________ Signature _________________________ Date