Frist Clinic – New Patient Medical History Intake Sheet
advertisement

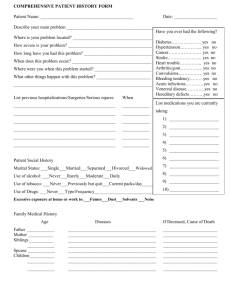
P PLLA AC CE ES STTA AM MP PH HE ER RE E Form # ENDOCRIN-2792 –FFE Orig 09/09 Comprehensive Patient History Form Page 1 Patient Name:_________________________________ DOS:_________________ DOB: _____________ Describe your main problem ____________________________________________________________________________________ Where is your problem located?____________________________________________ How severe is your problem? ______________________________________________ How long have you had this problem?________________________________________ When does this problem occur?_____________________________________________ Where were you when this problem started? __________________________________ What other symptoms happen with this problem?__________________________________ ______________________________________________________________________ List previous hospitalizations/Surgeries/Serious Injuries When? What makes this problem worse or better? ____________________________________ ________________________________________________ ____________________ ______________________________________________________________________ ________________________________________________ ____________________ ________________________________________________ ____________________ ________________________________________________ ____________________ ________________________________________________ ____________________ ________________________________________________ ____________________ Have you ever had the following? Diabetes………………. Hypertension…………. Cancer………………… Stroke…………………. Heart trouble………….. Arthritis/gout…………. Convulsions…………… Bleeding tendency…….. Acute infections……….. Venereal disease………. Hereditary defects……... yes yes yes yes yes yes yes yes yes yes yes no no no no no no no no no no no List Medications you are currently taking 1)_____________________________ 2)_____________________________ 3)_____________________________ 4)_____________________________ 5)_____________________________ Patient Social History 6)_____________________________ Marital Status: ❏ Single ❏ Married ❏ Separated ❏ Divorced ❏ Widowed 7)_____________________________ Use of alcohol: ❏ Never ❏ Rarely ❏ Moderate ❏ Daily _________________ 8)_____________________________ Use of tobacco: ❏ Never ❏ Previously but quit ❏ Current packs per day ______ 9)_____________________________ ❏ Never ❏ Type/Frequency_____________________________ 10)____________________________ Use of Drugs: Excessive exposure at home or work to: ❏ Fumes ❏ Dust ❏ Solvents ❏ Noise ❏ Chemicals Family Medical History Age Diseases If Deceased, Cause of Death Father _____ ________________________________________________________ ____________________________ Mother _____ ________________________________________________________ ____________________________ Siblings _____ ________________________________________________________ ____________________________ _____ ________________________________________________________ ____________________________ Spouse _____ ________________________________________________________ ____________________________ Children _____ ________________________________________________________ ____________________________ _____ ________________________________________________________ ____________________________ _____ ________________________________________________________ ____________________________ _____ ________________________________________________________ ____________________________ Page 2 Form # ENDOCRIN-2792-FFE Orig 10/09 PLEASE ANSWER ALL QUESTIONS Have you had any of the following during the past three months? CONSTITUTIONAL Good general health lately…………………….. Recent weight change…………………………. Fever…………………………………………... Fatigue………………………………………… Headaches……………………………………... No No No No No Yes Yes Yes Yes Yes EYES Eye disease or injury………………………….. Wear glasses/contact lens…………………….. Blurred or double vision……………………… Glaucoma……………………………………... No No No No Yes Yes Yes Yes ENT Hearing loss…………………………………... Ringing in the ears……………………………. Earaches or drainage………………………….. Sinus problems………………………………... Nose bleeds…………………………………… Mouth sores…………………………………… Bleeding gums………………………………… Bad breath or bad taste………………………... Sore throat or voice change……………………. Swollen glands in neck………………………… No No No No No No No No No No Yes Yes Yes Yes Yes Yes Yes Yes Yes Yes CARDIOVASCULAR Heart trouble…………………………………… Chest pains…………………………………….. Sudden heart beat changes…………………….. Swelling of feet, ankles or hands……………… No No No No Yes Yes Yes Yes RESPIRATORY Frequent coughing……………………………... Spitting up blood………………………………. Shortness of breath…………………………….. Asthma or wheezing…………………………… No No No No Yes Yes Yes Yes GASTROINTESTINAL Loss of appetite………………………………… Change in bowel movements………………….. Nausea or vomiting……………………………. Frequent diarrhea………………………………. Painful bowel movements or constipation…….. Blood in stool………………………………….. Stomach pain…………………………………… No No No No No No No Yes Yes Yes Yes Yes Yes Yes GENITOURINARY Frequent urination……………………………… No Yes Burning or painful urination…………………… No Yes Blood in urine………………………………….. No Yes Change of force of strain when urinating……… No Yes Incontinence or dribbling………………………. No Yes Kidney stones………………………………….. No Yes Sexual difficulty……………………………….. No Yes Male – testicle pain…………………………….. No Yes Female – pain with periods…………………….. No Yes Female – irregular periods……………………… No Yes Female – vaginal discharge…………………….. No Yes Female – # pregnancies _____ # miscarriages ______ Female – date of last pap smear ___________________ Female – findings of last pap smear ❏ Normal ❏ Abnormal Date: ______________________ Patient Signature: ___________________________________ MUSCULOSKELETAL Joint pain……………….……………………… Joint stiffness or swelling……………………… Weakness of muscles or joints………………… Muscle pain or cramps………………………… Back pain………………………………………. Cold extremities………………………………... Difficulty in walking…………………………… No No No No No No No Yes Yes Yes Yes Yes Yes Yes SKIN Rash or itching…………………………………. Change in skin color…………………………… Change in hair or nails…………………………. Varicose veins………………………………….. Breast pain……………………………………… Breast lump…………………………………….. Breast discharge………………………………… No No No No No No No Yes Yes Yes Yes Yes Yes Yes NEUROLOGICAL Frequent or recurring headaches………………... No Light headed or dizzy…………………………... No Convulsions or seizures………………………… No Numbness or tingling sensations……………….. No Tremors………………………………………… No Paralysis………………………………………... No Stroke…………………………………………… No Head injury……………………………………… No Yes Yes Yes Yes Yes Yes Yes Yes PSYCHIATRIC Memory loss or confusion……………………… Nervousness……………………………………. Depression……………………………………… Sleep problems…………………………………. No No No No Yes Yes Yes Yes ENDOCRINE Grandular or hormone problem………………… Thyroid disease………………………………… Diabetes………………………………………… Excessive thirst or urination…………………… Heat or cold intolerance……………………….. Dry skin………………………………………... Change in hat or glove size……………………. No No No No No No No Yes Yes Yes Yes Yes Yes Yes HEMATOLOGIC/LYMPHATIC Slow to heal after cuts…………………………. Easily bruise or bleed………………………….. Anemia…………………………………………. Phlebitis………………………………………… Past transfusion………………………………… Enlarged glands………………………………… No No No No No No Yes Yes Yes Yes Yes Yes ALLERGIC/IMMUNOLOGIC History of skin reaction or other adverse reactions to: Penicillin or other antibiotics………… No Yes Morphine, Demerol or other narcotics.. No Yes Novocaine or other anesthetics………. No Yes Aspirin or other pain remedies………. No Yes Tetanus antitoxin or other serums…… No Yes Iodine, methiolate or other antiseptic… No Yes Other drugs/medications ______________________________ __________________________________________________ Known food allergies _________________________________ Physician Signature: ______________________________________