Health Questionairre page 2 (English)
advertisement
")
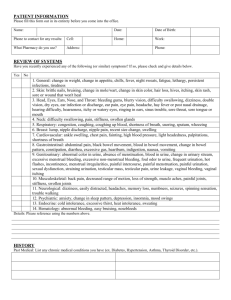
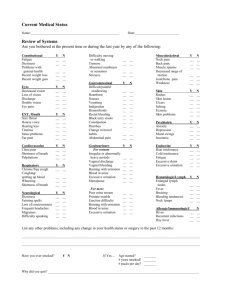
HEALTH QUESTIONNAIRE (Continued) ARE YOU EXPERIENCING ANY OF THE FOLLOWING: CONSTITUTIONAL SYMPTOMS GENITOURINARY Unexplained weight gain or loss ……………. Fever or chills ……………………………………….. Night sweats/Hot flashes ………………………. Fatigue ………………………………………………….. Yes Yes Yes Yes No No No No HEMATOLOGIC/LYMPHATIC Bleeding or bruising tendency ………………. Yes Anemia …………………………………………………. Yes No No EYES Blurred or double vision …………………………. Yes No EARS/NOSE/MOUTH/THROAT Hearing loss or ringing …………………………. Earaches or drainage ……………………………. Chronic sinus problem or rhinitis …………. Recurrent nose bleeds …………………………. Bleeding gums ……………………………………… Sore throat or voice change (hoarseness). Hay fever ………………………………………………. No No No No No No No Yes Yes Yes Yes Yes Yes Yes CARDIOVASCULAR Heart trouble ………………………………………… Yes Chest pain or angina pectoris ……………….. Yes Palpitation (fast or irregular heart beat) .. Yes Shortness of breath while walk/lying flat . Yes Swelling of feet, ankles or hands …………… Yes High blood pressure ………………………………. Yes No No No No No No RESPIRATORY Chronic or frequent coughs ………………….. Spitting up blood ………………………………….. Shortness of breath ……………………………… Asthma or wheezing …………………………….. No No No No Yes Yes Yes Yes GASTROINTESTINAL Loss of appetite ……………………………………. Yes Change in bowel movements ………………. Yes Nausea or vomiting ……………………………… Yes Frequent diarrhea ……………………………….. Yes Painful bowel movements or constip……. Yes Rectal bleeding or blood in stool …………. Yes Abdominal pain or heartburn ………………. Yes Peptic ulcer (stomach or duodenal) …….. Yes Trouble swallowing ……………………………… Yes Physician Initials: ______________ Date: ______________ No No No No No No No No No Frequent urination ……………………………Yes Burning or painful urination ……………..Yes Blood in urine ……………………………………Yes Urination at night (> 1/night)? ………….Yes Incontinence or dribbling ………………… Yes Decrease in urine stream ………………… Yes Kidney stones ………………………………….. Yes No No No No No No No Sexual difficulty ……………………………….. Yes Slow to start/stop urination …………….. Yes No No MUSCULOSKELETAL Joint pain ……………………………………….. Yes Joint stiffness or swelling ……………….. Yes Back pain ……………………………………….. Yes No No No INTEGUMENTARY (skin, breast) Rash or itching ………………………………... Yes Breast pain ……………………………………… Yes Breast lump …………………………………….. Yes Breast discharge ……………………………… Yes No No No No NEUROLOGICAL Frequent or recurring headaches …… Yes Lightheaded or dizzy ………………………. Yes Convulsions or seizures ………………….. Yes Numbness or tingling sensations ……. Yes Paralysis …………………………………………. Yes Memory loss or confusion ………………. Yes No No No No No No ENDOCRINE Thyroid disease ………………………………. Yes Diabetes …………………………………………. Yes Other glandular or hormone problem Yes No No No OTHER Nervousness …………………………………… Yes Depression/Anxiety/Panic ……………… Yes Insomnia ……………………………………….. Yes No No No Other concerns not noted above: ______________________________________ ______________________________________ ______________________________________ _______________________________________