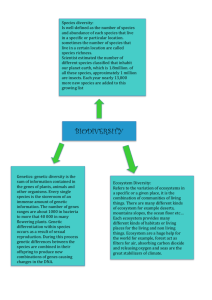
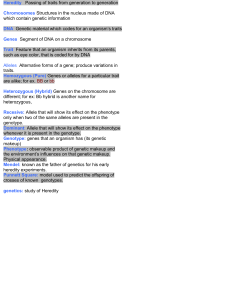
The Genetics of Child Development I. GENETIC FOUNDATIONS A. The Genetic Code l. Chromosomes: "colored bodies" carrying genetic material contained in the nucleus of all cells except red blood cells Humans have 23 pairs (n = 46) Chimpanzees have 24 pairs Horses have 32 pairs Mice have 20 pairs 2. Genes: multiple genes per chromosome; most genes lead to production of some protein. Genes composed of: 1 3. DNA (deoxyribonucleic acid): genes differ in length of the segments of DNA --Double helix structure (twisted ladder); uncoiled set of 23 chromosomes would be 3 feet long (in each cell) --Sides of ladder: alternating sugar and phosphate molecules in two threads wound around each other. --Ladder rungs consist of pairs of nucleotides (nitrogen-based molecules) attached to the sugar units of the sides: Adenine (A) paired with Thymine (T) Cytosine (C) with Guanine (G) --sequence of pairings determines the genetic instructions --chromosome 1 has 263 million bases; smallest (chrom. 21) has 50 million bases (Human Genome project) 2 4. Karyotype: depicts homologous pairs (except for the XY pair in males)--in humans, 22 of the pairs are known as autosomes, and l pair are sex chromosomes. 5. Gametes: sex cells (egg, sperm) contain only 23 chromosomes each 6. Mitosis: process by which DNA duplicates itself --DNA ladder splits down the middle, leaving each exposed base free to pick up its complementary mate from the cell cytoplasm --sister chromatids attached at centromere then separate during cell division e.g., Zygote (fertilized egg) replicates in first 24 hours 3 7. Meiosis: process by which gametes, or sex cells are formed --Cell with 46 chromosomes replicates itself (but doesn't split from sister chromosome) --Crossing Over: pairs of chromosomes exhange corresponding segments to create new genetic combinations --Cell then divides, then divides again to leave 4 cells with 23 chromosomes each 8. Alleles: the different forms/versions of each gene (e.g., Brown-eye, blue-eye, green-eye, etc.) --occur at the same locus on the autosomes, one each from mother and father 4 9. Genotype: one's genetic inheritance (e.g., BB or Bb or bb for eye color) homozygous: having same two alleles for a trait (e.g., BB or bb) heterozygous: having two different alleles for a trait (e.g., Bb) 10. Phenotype: one's expression of a trait (e.g., Brown eyes vs. blue eyes) 11. Monozygotic Twins share a genotype (mono- = one zygote); dizygotic (fraternal) twins do not 5 II. GENETIC INHERITANCE A. Autosomes: 1. Dominant Traits: supercede expression of recessive traits 2. RecessiveTraits: Exhibited only when inherit two alleles (only one allele makes one a carrier) Dominant Recessive Brown eyes Gray, green, blue Curly hair Straight hair Brown hair blond or light hair Non-red hair (BR,bl) Red hair thick lips thin lips dimples no dimples farsightedness normal vision Rh-positive blood Rh-negative blood 6 3. Co-dominance: With some traits, a combination of the alleles is phenotypically expressed, as with AB blood. Dominant Recessive Type A blood Type O Type B blood Type O 4. Polygenic inheritance: More than one gene influences expression of a trait, such as intelligence and height 7 5. Dominant & Recessive disorders: a. Dominant --Huntington's chorea: occurs 35-40 years of age, causes brain deterioration loss of motor control, memory, personality, etc. --Familial Alzheimer's --Marfan's syndrome b. Recessive --Albinism --Congenital deafness 8 --PKU, or phenylketonuria (chrom. 12) 1 in l0,000 births lack the ability for the liver to produce the enzyme phenylalanine hydroxylase, that converts a amino acid phenylalanine into tyrosine toxic excess of phenylalanine builds up in nervous system, leading to symptoms by 3-5 months; death by 4 without dietary restrictions phenylalanine is amino acid in protein, and is found in milk products, eggs, meat, poultry, legumes, nuts, wheat & oats 9 --Galactosemia (chr. 9, 17, 1—depends on enzyme missing) lack enzyme to convert galactose (from lactose in milk) into glucose. Buildup in tissues causes mental retardation, cataracts, enlarged liver, & kidney failure Detection prenatally + newborn --Cystic Fibrosis (chrom. 7) most common genetic disease among Caucasians (1 in 3000; 4-5% of Americans are carriers; caused by a change in single nucleotide, or one letter error) respiratory tract becomes clogged with mucus, increases risk of infection (death by mid-20s) secretions also obstruct pancreas, leading to dietary problems; salty tasting skin 10 --Tay-Sachs disease (chrom. 15) highest incidence in Ashkenazic Jews mental retardation, blindness, deafness, and paralysis begin around 6 months of age; death normally occurs by 3-4 years due to absence of an enzyme, Hex-A (Hexosamindase-A), which allows a lipid to accumulate in brain --Sickle cell anemia (chrom. 11) incidence highest in African/Americans caused a change in a single amino acid in hemoglobin, which prevents some blood cells from carrying oxygen, leading to a crescent shape Oxygen depletion from exercise, plane cabins, etc. leads to painful sickling of blood cells. Heterozygotes show protection from malaria. 11 B. Sex-linked Inheritance 1. Y-linked Inheritance: --Hairy ears 2. X-linked Inheritance: often recessive genes on X-chromosome Males have higher probability of phenotypic expression than females. --Red-green color blindness --Hemophilia (detectable prenatally) --Duchenne muscular dystrophy --Lesch-Nylan disease buildup of uric acid leads to accumulation of salt crystals in CNS, joints, kidneysrecurrent vomiting, cerebral palsy, mental retardation, self-mutilation & death 12 --Fragile X Syndrome: a genetic disorder resulting in multiplication of part of genetic code, resulting in a “pinched” long leg on the X-chromosome -on long arm of X, the triplet CAG replicated 20-30 times; if replicated over 50 times (up to 200), leads to Fragile X-type symptoms (DeSalle & Lindley, 1997) incidence in 1 in 1000 births most common genetic form of mental retardation 13 facial deformities (large ears, prominent jaw, long narrow face), and large testes in males affected females may show reduced intelligence, though most are normal possible link to infantile autism 14 Food for thought: Male fetuses are more likely than female fetuses to be aborted, stillborn; infant and childhood mortality is greater for males, as is the rate of learning disabilities, behavioral disorders, and mental retardation. This may be due to genetic disorders (especially X-linked). However, a greater number of boys are conceived, and there are l06 male births for every l00 females. 15 III. CHROMOSOMAL ABNORMALITIES Risk factors: Advanced Maternal Age (sometimes advanced Paternal age) --many caused by a glitch in meiosis http://gslc.genetics.utah.edu/units/disorders/karyotype/ A. Autosomal Abnormalities l. Down's Syndrome (Trisomy 2l) --Incidence: 1/700 live births 16 --Physical features: ipicanthal fold of eye, flattened facial features, poor muscle tone, short stature, and short broad hands with an unusual crease in palms; excess skin on back of neck --Internal traits: congenital heart defects, cataracts/visual impairments, deficiencies in immune system leading to susceptibility to infection and leukemia --Shortened life expectancy; those who live to over 35 typically develop the same neuro-physiological and -psychological symptoms as Alzheimer's patients 17 --Cause: failure of chromosome 2l to segregate during meiosis. Down's syndrome children show a mosaicism-extra chromosomal material appears in only some cells; degree of impairment related to number of cells affected. --Theories: Older Egg vs. “Relaxed Selection” hypotheses. 18 2. Edward’s Syndrome (Trisomy 18) --Incidence: 1/5000-6000 live births; predominantly females --80-90% mortality rate by age 2 --Severe mental retardation; elfin facial features (small nose & mouth, receding chin, abnormal ears); hearing loss; seizures; hypoglycemia 19 20 3. Patau Syndrome (Trisomy 13) --Incidence: 1/20,000 live births --High mortality rate in 1st year --Cleft lip & palate; congenital heart defects; polydactyl; severe mental retardation 21 22 4. Cri-du-Chat (missing short arm of chr. 5) --Incidence: 1 in 50,000 births; Possibly normal life expectancy. --Catlike cry; microencephaly; congenital heart disease; severe mental retardation; may be missing kidney/s; sensitivity to loud noises; low birth weight, partial webbing of fingers or toes --later, protuding teeth (normal sized teeth in small head); curvature of spine; developmental & language delays; possibly self-mutilation & rocking 23 B. Sex Chromosome Disorders l. Turner Syndrome: X0 --Females in which one X-chromosome (or part of it) is missing. Incidence: l in l200-2500 females (90% are spontaneously aborted). --May not be detected until puberty, when secondary sex characteristics & menstruation do not develop. 24 --Ovaries do not develop prenatally, the girls maintain a very immature appearance: Short stature (57 inches average), a webbed neck. Increased risk of fractures, strokes, diabetes & cardiovascular problems. --Hormone therapy may increase height and induce menstruation; occasionally pregnancy accomplished through in vitro fertilization. --Intelligence is often near average, although with severe deficits in spatial ability and directional sense (perhaps due to smaller amounts of brain tissue— grey & white--in parietal lobes; Reiss, 1995). 25 2. Triple X Syndrome: XXX Incidence: 1 in 500-1200 female (?) --Normal sexual development --delays in language development, lack of motor coordination, poor academic performance, and immature behavior. 26 3. Klinefelter's Syndrome: XXY males --Incidence: One in every 500-l000 births --absence of development of male secondary sex characteristics (facial hair, deepening voice, increased muscle structure) at puberty. 27 --Underdeveloped testes & sterile (may institute hormone therapy); Female-like fat distribution, and potential breast development at puberty 28 --Tall, and tend to be overweight. --Cognitive deficits: expressive language delays in development, poor auditory STM, reading difficulties, about 20% have mild to moderate retardation --self-esteem problems; prefer quieter pursuits 29 4. Jacob’s Syndrome: XYY --Incidence: One in 2000 males. --Above-average height, large teeth, and sometimes severe acne --Overrepresented in prison populations (popular defense for a while), but not necessarily more aggressive [Representation in prisons possibly due to decreased intelligence 30 IV. METHODS OF PRENATAL TESTING A. Non-invasive techniques 1. Genetic Counseling --Information on a person's family tree is gathered to ascertain the risk of certain diseases. --Genetic screening can be carried out on parents to determine their genotype for given disorders (e.g., Cystic Fibrosis, Tay Sachs, sickle cell anemia). 31 2. Triple Screen Test (15th-16th medical weeks, up to 18th) --Maternal blood test measures: Alpha-feta protein (from fetal liver) Estriol hCG (human Chorionic Gonadotropin) (inhibin A—increases detection of Down’s) --high levels of Alpha-feta protein may indicate neural tube defect (or baby is older than thought, or (!) twins). 75-85% detection --high levels of hCG, with low levels of estriol & AFP, indicate elevated risk for Down’s Syndrome. 60% detection in women < 35; 75% in women > 35 --low levels of all 3 may indicate higher risk for trisomy 18 Edward’s syndrome) --HIGH risk of “false positive” (46% in an online poll of 23, 470 parents), and some risk of false negatives 32 3. Ultrasound (up to delivery) --High frequency sound waves are beamed into the uterus, and their reflection reveals the size, shape, and position of the fetus. --a STRUCTURAL measure used to monitor fetal growth, estimate gestational age, detect multiple pregnancies, depict placement of placenta, and detect gross structural abnormalities --can be done abdominally or transvaginally Figure 1 - Fetus with subcutaneous collection of fluid at the back of the neck (often seen in Down’s Syndrome fetuses & those with other trisomies). Image kindly provided by Dr Eva Pajkrt, University of Amsterdam. 33 --growth abnormalities sometimes indicative of genetic & chromosomal abnormalities --historically, has been claimed that there are no known risks. However, several studies in 1990s found: -increase in left handedness in men, indicating subtle brain damage (32% increase with two pregnancy scans; Swedish study) 34 --cell damage due to : -tissue heating (Uhlig, 1999) -cavitation—sound waves may cause bubbles to form & expand --reduced fetal weight, fetal organ weight, birth rate, decreased immune system functioning, problems with blood platelets, have been noticed in humans & other species exposed to ultrasound http://educate-yourself.org/cn/2001/ ultrasoundandbraindamage19dec01.shtml B. Invasive Techniques *Usual analysis is for Chromosome abnormalities; genetics analysis done only if risk factors for a disease are present --95% of fetuses examined are normal 35 1. Chorionic Villa Sampling (10-13 medical weeks) --Chorion is the fetal membrane that will form the fetal side of the placenta --a tissue sample is removed from chorion by pushing narrow needle in 15-20 times --Complications: -1-2% risk of inducing miscarriage -may interfere with vascularization --> limb deformities -Mosaicism a problem for females 36 2. Amniocentesis (14-16th medical weeks) --Fetal cells are extracted from the amniotic fluid and cultured for chromosome/genetic analysis --Complications: -Risk is .33-.5% (1/300 to 1/200) for inducing miscarriage [hence benchmark of age 35, where risk of any chromosome abnormality is 1/180] -Risk is even higher with early amniocentesis (11-14th weeks) -Rh- mothers need Rhogam because of risk of co-mixing blood of mother & baby 37 3. Fetoscopy (18-22 medical weeks, or after 16th) --miniature telescope-like instrument w/ light & lenses inserted into tiny incision into amniotic sac --can detect structural deformities --Blood samples taken from junction of umbilical cord/placenta, and/or tiny bit of fetal or placental tissue removed --Complications: -up to 12% risk of inducing miscarriage -up to 47% risk of rupturing membranes, necessitating pre-term delivery -Rh- mothers need Rhogam risk of co-mixing blood of mother & baby 38 V. HEREDITY INFLUENCES on BEHAVIOR A. Estimating Hereditability 1. Hereditability refers to the extent that individual differences within some population are due to genetics (e.g., hereditability for having 2 eyes is 0.00—having two eyes is clearly based on genes, but no individual differences) 2. Concordance Rates & Correlations --Determine hereditability by measuring a trait in individuals with shared genes and/or shared environments: Biological parents, siblings Identical twins, raised together or apart Fraternal twins, raised together or apart Adoptive parents & adopted child Biological parents & adopted child 3. What does the Correlation mean? Correlation of r = 0.70; if squared, provides amount of variance due to genetics = .49 (or 49%) 39 4. Many personality traits (e.g., Intro/Extroversion & Empathy) and Intellectual Traits/skills clearly have an inherited component. Average Correlations between IQ scores (Bouchard & McGue, 1981; *Pederson et al, 1985; **Segal, 2000) Family Pairs Identical Twins Raised Together .86 Raised Apart .72 Fraternal Twins .60 .52* Biological Siblings .47 .24 Biological Parent & Child .42 .22 Half Siblings .31 -- Adopted Siblings .34 -- Adoptive Parent & Adopted Child .19 -- Unrelated siblings (same age, same home) .26** -- Hereditability of Temperament: Correlations of Angry Emotionality (Plomin et al., 1988) Raised Together Raised Apart Identical Twins .37 .33 Fraternal Twins .17 .09 40 Hereditability of Certain Traits from Minnesota Twin Study (Bouchard et al., 1990) 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 Heig. Weig. S ys. BP IQ Person. Relig. S oc. Att. Height Syst. BP Personality Social Attitudes Weight IQ Religiosity 41 5. However, environment also impacts almost all inherited skills or traits. Gene Environment Interactions: Odds of Depression at age 26 (Caspi et al., 2003) 0.45 0.4 0.35 0.3 2 hi-risk genes Heterozygous 2 protective genes 0.25 0.2 0.15 0.1 0.05 0 0 1 2 3 4 Number of Stressful Childhood Events 42 B. Interaction of Genes & Environment l. Canalization (Conrad Waddington): the degree to which a trait is constrained by genetics. Some traits (e.g., crawling) more canalized than others (e.g., playing soccer). Think of a river (a child's development) seeking its course over terrain. Deeply canalized sections will mold the river; shallower sections will be molded BY the river. Some traits may be heavily canalized early in development (e.g., language development), but less so later on (e.g., reading ability). 2. Range-of-Reaction (Gottesman, 1963): Genes set boundaries & establish a range of reactions; because of different genotypes, individuals will respond differently to the same environment 43 3. Niche-picking (Scarr & McCartney, 1983): Genotype contributes propensities toward certain skills and abilities, and we then seek activities which are compatible with our genetic endowment. (Active Genotype/Environment interaction) 4. Correlations between genetics and environment can also occur: a. Passively, as when parents set up an environment consistent with their (and their child's) predispositions (e.g., sociability); or b. Evocatively, as when a child’s traits influence the behavior of those around him/her (e.g., if a shy child is less engaged) 44
 0
0
advertisement
Related documents



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users