- Organ Donation Alliance
advertisement

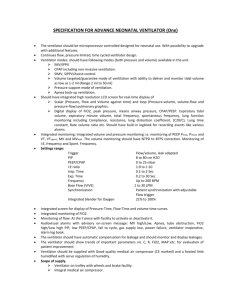
Ventilator Management Orders For Consented Organ Donors ______BiLevel Set Up Initial FiO2 40% Rate 8 - 20 PEEP Low 10 – 18 cm H2 : Adjust to maintain PaO2 > 100 mm Hg on FiO2 40% PEEP High to obtain Vt 6 - 10 ml/kg ideal body weight Adjust TH (time at PEEP high) to maintain an initial I:E 1:1 Monitor closely, maintaining PIPs < 38 cm H2O Keep I:E ratio as close to 1:1 as possible while avoiding Auto peep BiLevel Ventilation Changes – as indicated per ABG’s To increase ventilation (ie decrease PaCO2) while maintaining MAP Increase rate: Adjust TH (time at PEEP High) to maintain 1: 1 ratio OR Increase PEEP High keeping Vt 6-10 ml/kg ideal body weight To decrease ventilation (ie increase PaCO2) while maintaining MAP Decrease rate: Adjust TH (time at PEEP High) to maintain 1:1 ratio OR Reduce PEEP High keeping Vt 6-10 ml/kg ideal body weight To increase oxygenation (ie increase PaO2) Keeping FiO2 at 40% Raise Peep Low and raise the PEEP High by the same amount keep PIP’s < 38 OR Increase the I:E ratio (lengthen the TH) DO NOT inverse I:E ratio without speaking to LifeShare Coordinator ______Pressure Control Set Up (for Transport Ventilators or when BiLevel is not available) Initial FiO2 40% Rate 8 – 20 PEEP 10 – 18 cm H20: Adjust to maintain PaO2>100 mm Hg on FiO2 40% Inspiratory Pressure set to obtain Vt 6 - 10 ml/kg ideal body weight Adjust Inspiratory time to maintain an initial I:E 1:1 Monitor closely, maintaining PIPs < 38 cm H2O Keep I:E ratio as close to 1:1 as possible while avoiding Auto peep Pressure Control Ventilation Changes as indicated per ABG’s To increase ventilation (ie decrease PaCo2) while maintaining MAP Increase rate: Adjust I time to maintain 1:1 ratio OR Increase Inspiratory pressure keeping Vt 6 - 10 ml/kg ideal body weight To decrease ventilation (ie increase PaCO2) while maintaining MAP Decrease rate: Adjust I time to maintain 1:1 ratio OR Decrease Inspiratory pressure keeping Vt 6-10 ml/kg ideal body weight To increase oxygenation (ie increase PaO2) keeping FiO2 at 40% Increase PEEP keeping the PIP’s<38 DO NOT inverse I:E ratio without speaking to LifeShare Coordinator _______Respiratory Therapy Orders Verbally report all ABG results, documenting MAP and Plateau Pressure, and ventilator changes to LifeShare Coordinator Use a heated circuit and DO NOT disconnect patient from ventilator without LifeShare notification Place an end tidal CO2 or transcutaneous CO2 monitor and correlate with ABG’s Transport ventilator to be used for all trips In the event a transport ventilator is not available, manual ventilation with a PEEP valve is REQUIRED Verify respiratory therapy orders on Adult Order Set and confirm chest PT Oxygen Challenge (complete as ordered) Obtain a baseline ABG prior to making ventilator changes for O2 challenge, documenting MAP and Plateau Pressure Maintain BiLevel or PCV mode during challenge Increase FiO2 to 100% Decrease PEEP Low to 5 cm H2O BiLevel - decrease PEEP High to maintain Vt prior to O2 Challenge Pressure Control - adjust inspiratory pressure to maintain Vt prior to O2 Challenge Maintain setting for 15 minutes Draw ABG, documenting MAP and Plateau Pressure, then immediately return to previous settings Verbally report to LifeShare Coordinator ABG’s and then make changes as indicated by previous ABG Signature:_____________________________________________ per LifeShare Standing Orders/Protocol LifeShare Organ Recovery Coordinator Date:___________________ Time:__________________ Reviewed Date 02/22/2010 Lung Management Guidelines for LifeShare Coordinators – pg 1 Not part of order set Upon consent and prior to ANY vent changes, consider a baseline ABG and O2 challenge Initiate Ventilator Management Orders for ALL consented brain dead organ donors In DCD, the attending physician has to sign the order for vent changes, but we do recommend it Verify orders placed for: 1. Stat chest x-ray now and q 6 hours Lung measurements of initial CXR and hard copy of terminal chest x-ray 2. ABG’s/O2Challenge prn with initial changes and then q 2 hours As directed by LifeShare ALL ABG’s verbally reported to LifeShare Coordinator 3. Bronchoscopy for both anatomical and therapeutic evaluation Minimal lavage Separate culture and smears from each lung, if possible Repeat O2 Challenge 1 hour after bronchoscopy 4. Echocardiogram Consider reducing the low PEEP to 8 for ECHO and returning to previous settings when complete Question if a poor echo is due to increased intrathoracic pressures if Peep >10 Verify medications ordered on Routine Deceased Donor Orders: 1. Narcan 8 mg IVP – USE EARLY/USE ALWAYS 2. SoluMedrol 2 gm and repeat 1 gm q 12 hours 3. Zosyn 4.5 gms IV STAT and repeat q 6 hours Consider use of these additional medications as indicated: 1. Bronchodilators - Combivent MDI or Albuterol MDI 10-12 puffs every 2-4 hours Avoid nebulizers, they place a break in the circuit 2. Vasopressin infusion titrated to desired urine output Wean Levophed off first, titrating Neosynephrine and Dopamine down as tolerated Consider d/c if hemodynamically stable 1-2 hrs prior to OR to allow natural diuresis 3. Dopamine – recommended/”acceptable” dose 3 mcg/kg/min If pt requires pressor support, this is first line preference of transplant surgeons in general 4. Mannitol 25-50 gm bolus, then consider infusion of 3-6 gm/hr Mechanism allows for “third space” fluid to be diuresed and protection of lungs Closely 1. 2. 3. Verify orders and review with RN and respiratory therapy for aggressive pulmonary toileting, which may include any or all of the following: 1. Module bed with rotation and percussion Notes on Chest PT Percussion 15 min q 1 hours (minimum) -Evaluate chest Xray prior to initiating Manually Rotate pt > 45 degrees q 1 hour percussion to evaluate for rib fxs, etc Module bed rotation q 15 minutes -Maintain pt in high lateral position 2. Manual percussion/pulmonary therapy (consider if module not available) -If module or rotation bed used, manually Percussion q 2 hrs – consider LINK vest rotate the patient to > 45% angles hourly Manually rotate hourly -Rotation should always be right to left, left 3. Suction with gentle quad cough to right, NEVER flat on the back If you auscultate sounds after percussion, suction -Percuss only one side at a time to minimize time in trendelenburg If no sounds or secretions, suction q 4 hrs 4. Auscultate q 2 hours 5. HOB elevated @ 30° (except during manual CPT and suctioning trendelenburg) Adjust vent setting per ABG’s, as indicated Correlate ABG’s with end tidal CO2 device Expect a 7 point variation, anything greater is indicative of how sick your patient may be monitor/achieve/maintain hourly: CVP 4-8 mmHg I and O status Adjust fluids as necessary to maintain CVP and clear lung fields Avoid albumin Remain conscious of vasopressin dosing Reviewed Date 02/22/2010 Lung Management Guidelines for LifeShare Coordinators – pg 2 Not part of order set After evaluating social/medical history, ABG’s, chest x-rays and bronchoscopy, consider chest CT ONLY after discussion with AOC and Intensivist consult Verify pt has not already had one done upon admission Allocation decision: 1. If Pa02 >350 and CXR clear or improving Begin placement 2. If Pa02 <350 and/or CXR not clear, worsening: Reconsider: a. Bronchodilators every 1 hour X 2 b. Mannitol bolus/gtt c. Aggressive pulmonary toilet d. Ventilator manipulation and/or other recruitment maneuvers e. Repeat therapeutic bronchoscopy Discuss with AOC and Intensivist stopping pursuit of lungs If lung allocation stopped: D/C serial CXR’s and ABG’s except as needed for overall management IMPORTANT/FYI: Sputum Gram Stain Characteristics Clinical Interpretation Large number of squamous cells, few to moderate PMN’s Saliva, possibly mixed with purulent (polymorphonuclear cells), mixed flora bronchial secretions Large number of PMNs; gram positive diplococci Pneumococcal infection Large number of PMNs; gram negative organisms Haemophilis infection Large number of PMNs; gram positive cocci in clusters Staphylococcal infection Large number of PMNs; no organisms seen Transport ventilators are necessary for all “trips” and settings should be discussed with intensivist, respiratory therapist, anesthesia and LifeShare Coordinator if BiLevel is not available Avoid disconnecting patient from ventilator or any interruptions in the circuit The Ventilator Management Orders is acceptable in pediatrics. You may need to reevaluate the Rate, PEEP and PIP. The acceptable parameters will be established on a case by case basis. Reviewed Date 02/22/2010