The Case of the Man Who Began Tripping on the Carpet
advertisement

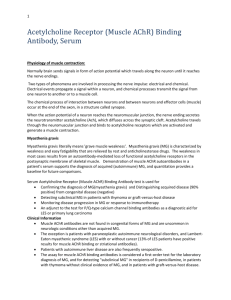
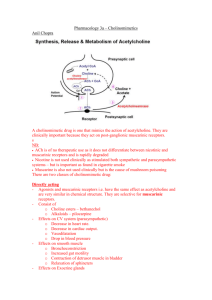
A&P 11-12 Name ____________________________ The Case of the Man Who Began Tripping on the Carpet Learning Objectives 1. 2. 3. 4. Describe the normal sequence of events for nerve cell stimulation of a muscle cell. Explain the function of acetylcholine and acetylcholine esterase. Describe the main molecular defect in myasthenia gravies. Explain the physiological basis for diagnosing and treating myasthenia gravis with acetylcholine esterase inhibitors. 5. List at least three physiological signs (for example, organ symptoms or signs) that would occur with damage to acetylcholine receptors on muscle. Case Presentation Dale Peterson, a 45-year-old grade school teacher, has experienced some serious physical changes in the last month. He noticed himself tripping on the carpet while walking; this really bothered him because he did not like to appear clumsy in front of his friends. Mr. Peterson also noticed occasional blurred vision and problems swallowing food. His wife, Linda, noticed that his eyelids seemed droopy. It was the blurred vision that caused Mr. Peterson to go to an ophthalmologist. The ophthalmologist, after examining Mr. Peterson and listening to his description of his recent problems, referred him to Dr. Erwin, and internist specializing in neuromuscular disorders. Dr. Erwin suspected that Mr. Peterson might have myasthenia gravies. Dr. Erwin examined Mr. Peterson, noting that his muscle strength was not bilaterally symmetrical, and that his muscle strength seemed weaker than normal for a 45-year-old male. To confirm his suspicions, Dr. Erwin gave Mr. Peterson a small dose injection of Tensilon, a reversible inhibitor of acetylcholine esterase. Mr. Peterson’s muscle weaknesses disappeared and the drooping of his eyelids went away. Blood was drawn and sent to the laboratory to test for the presence of antibodies to acetylcholine receptor proteins. Within the hour, Mr. Peterson’s muscle weakness reappeared. The laboratory test revealed the presence of antibodies against acetylcholine receptors. Dr. Erwin was all but certain that Mr. Peterson had myasthenia gravis. Dr. Erwin started Mr. Peterson on a drug treatment regimen of neostigmine, 30 mg PO (to be given orally) q (every) 4 hours, and prednisone 50 mg PO qod (every other day). Case Background Myasthenia gravis is a disorder in which muscle weakness occurs. The term myasthenia gravis literally translates as “muscle (myo-) weakness (asthenia) serious (grave)”. It is believed to be caused by an attack by the immune system against the acetylcholine receptors on the muscle cell membrane. To understand myasthenia gravis, it helps to review the normal physiology of muscle cell stimulation. Recall that the nerve cell to muscle cell releases the neurotransmitter acetylcholine (Ach), which binds to skeletal muscle Ach receptors, triggering muscle cell contraction. Acetylcholine esterase, present in the synapse, then degrades the Ach so that constant interaction between Ach and the muscle cell Ach receptors do not occur. With myasthenia gravis, immune system antibodies bind to the Ach receptors on the muscle cell, preventing normal interaction between Ach and the Ach receptor. A portion of the Ach receptors A&P 11-12 Name ____________________________ will have antibody bound to them; the remainder will still be available for interaction with Ach. The severity of myasthenia gravis will depend on the relative number of Ach receptors that are blocked by immune system antibody. Characteristically there are periods of remission, but the disease is usually progressive. Primarily it is skeletal muscle that is involved. Weakness of ocular muscles for eye movement leads to blurred vision. Weakness of leg muscles frequently leads to tripping as one attempts to walk. Involvement of the upper esophagus (containing skeletal muscle) can lead to problems swallowing food. Treatment, and also diagnosis, involves giving molecules (such as neostigmine) that bind to and inhibit the activity of acetylcholine esterase. With subsequent decreased activity of acetylcholine esterase, less destruction of Ach occurs. The result will be increased molecular interactions between Ach and available (unblocked) Ach receptors. Muscle cell contractions should be strengthened. In addition to treatment with acetylcholine esterase inhibitors, corticosteroids such as prednisone are used to inhibit the immune system. If the immune system is inhibited, the amount of antibody to Ach receptors that is produced should diminish. Questions 1. Describe the normal sequence of events and molecules involved for nerve stimulation of skeletal muscle cell contraction. 2. What is acetylcholine esterase? What is its purpose? 3. Curare poison, from the bark of a tree in South America, binds to Ach receptors but does not activate them. What effect will curare have on muscle tissue? 4. Organopesticides bind to acetylcholinesterase and inhibit its normal activity. What effect will organopesticides have on muscle tissue? 5. Botulism food poisoning, from a toxin secreted from the bacterium Clostridium botulinum, inhibits nerve cell release of acetylcholine. What effect will botulism food poisoning have on skeletal muscle tissue? What might ultimately kill someone poisoned with this toxin? 6. How might one treat myasthenia gravis? Explain the molecular basis for the treatment. 7. How might one treat poisoning from curare? Explain the molecular basis for the treatment.