(Attachment: 10)Report
advertisement
Report")
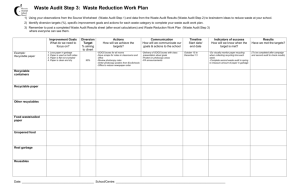
*PART 1 – PUBLIC DOCUMENT AGENDA ITEM No. 11 TITLE OF REPORT: DATA QUALITY IMPLEMENTATION UPDATE REPORT OF THE HEAD OF FINANCE, PERFORMANCE AND ASSET MANAGEMENT 1. SUMMARY 1.1 To provide the Committee with an update on the implementation of the Performance Combined Data Quality Improvement Plan. 2. FORWARD PLAN 2.1 This report does not contain a recommendation on a key decision and has not been referred to in the Forward Plan. 3. BACKGROUND 3.1 The former Audit and Risk Sub Committee received reports on the implementation of a Data Quality Improvement Plan. This was a number of actions arising from both Internal and External audits on Performance Indicators. 3.2 The last Internal Audit specifically on performance indicators was finalised in August 2009 and the finding was a “substantial” level of assurance (compared to “moderate” in the previous audit completed in November 2008). This latest audit coincided with the first full year of reporting under the new system of National Indicators and with the introduction of the Covalent performance management system. 3.3 The launch of Covalent as the Council’s performance and risk software, has introduced checks on the accuracy of data by the processes that are followed before the data becomes “live” on the system. 3.4 The most recent report on the implementation of this improvement plan was submitted to the Audit and Risk Sub Committee on 24th February 2010. At this meeting it was agreed that the action plan would be entered onto Covalent to improve the layout and facilitate the monitoring of the delivery of this plan. However, on reviewing the outstanding actions it was found that these were all complete and to enter them onto Covalent would not be of benefit. 3.5 Data Quality and Information formed a Key line of Enquiry in the Use of Resources assessment that was conducted by our external auditors. AUDIT AND RISK (15.9.10) 4. UPDATE ON OUTSTANDING ACTIONS 4.1 The last update report to the Audit & Risk Sub Committee, contained six outstanding improvement entries. Each entry referred to one or more internal audit recommendation. Five were categorised as being ‘on target’ and one was categorised as being ‘behind schedule’. 4.2 Rather than update the old action plan and attach this as an appendix, the original audit recommendations have been reviewed and progress on delivery of each of these is reported below. The Committee should note that the summary relating to information management addresses two related improvements. This report, therefore, details five summaries in total. 4.3 Information Management 4.3.1 One entry relating to the synergies between data quality and data protection / freedom of information, consisting of three internal audit recommendations, was ‘behind schedule’ at the time of the last update report. The three original audit recommendations were: Consideration be given to combining all areas involving data and information assurance to enable these issues to be given a greater prominence and priority throughout the authority; The Data Quality Forum and Information Assurance Group be combined; Consideration be given to combining all information related functions within the authority so that data quality, data protection and freedom of information, record storage and retention are encompassed within one section so that full use is made of the synergies and interconnections between them. 4.3.2 The Head of Information Technology & Customer Services has responsibility for information sharing, data protection, freedom of information, land and property data, GIS information and web content. He also works with the Head of Finance, Performance & Asset Management on the aspects of the retention schedule that have data protection implications. The Head of Information Technology & Customer Services has drafted an Information Management Strategy to show the links between these different aspects and how these areas may develop in the future. 4.3.3 The Head of Information Technology & Customer Services has circulated the draft Information Management Strategy to key staff and has received feedback on the content. He is now in the process of reviewing this feedback and producing a final version of the strategy for consideration by CMT. In summary, the Information Management Strategy addresses a number of issues including knowledge management, information management, data quality, data security and information assurance. For each of these, the strategy shows a position statement for the Council, along with a proposed way forward. These proposals form an action plan as an appendix to the strategy. AUDIT AND RISK (15.9.10) 4.3.4 The newly created Information Management Group will own the Information Management Strategy. This group provides an overview of information management and has membership from across the authority. It is the result of combining the Data Quality Forum and Information Assurance Group and has new terms of reference. The Information Management Group first met in May 2010 and the next meeting is planned for September. The proposal is that the group will meet on a quarterly basis and focus on elements of the Information Management Strategy to develop and manage the flow of information relating to information management within the Council. 4.3.5 Another factor is that as well as chairing the Information Management Group, the Head of Information Technology & Customer Services also chairs the Information Technology Transformation Board (ITTB). Aspects of information management that have technology requirements / impacts or vice versa are therefore now managed by one Head of Service. 4.3.6 In summary, the Head of Information Technology & Customer Services believes that the internal audit recommendations have been implemented. 4.3.7 The process of combining the Data Quality Forum and Information Assurance Group to form the new Information Management Group, has also addressed one further entry that was ‘on target’ at the time of the last update report. This internal audit recommendation was – ‘The effectiveness of the Data Quality Forum or the new merged group in championing data quality issues should be evaluated and the outcomes reported to CMT.’ 4.4 Data Quality Checks 4.4.1 One audit recommendation relating to the periodic checking of data was ‘on target’ at the time of the last update report. This recommendation was – ‘A series of checks should be performed periodically on the Covalent system. Internal Audit will assist the Performance Team in determining an appropriate set of checks if required.’ 4.4.2 The Performance & Risk Team developed a monthly procedure and checklist to address this recommendation and introduced it at the beginning of 2010/11. This involves checking that officers have published data on Covalent in a timely manner and in line with corporate guidance. 4.4.3 Each month, the Performance & Risk Team check whether Data Input Officers have entered corporate performance data onto Covalent and Data Activators have approved it, by the 28th of the following month. For example, officers were expected to have published July performance data on Covalent, by the 28th of August. The Performance & Risk Team report the results of these checks via two new management indicators: MI PT001 - The % of PI data added to Covalent on time MI PT002 - The % of PI data activated on Covalent on time 4.4.4 The monthly procedure also consists of further checks to ensure that officers have updated each performance indicator in line with corporate guidance. The full checklist consists of the following nine questions: 1. Has the data been loaded on time (28th)? 2. Has the data been loaded correctly? 3. Has the evidence been loaded or a filepath specified? AUDIT AND RISK (15.9.10) 4. Does the evidence support the data? 5. Does the evidence comply with Data Quality? 6. Is the evidence named correctly? 7. Is the evidence linked correctly? 8. Has the data been activated (28th)? 9. Have suitable notes been added when activated, if required? 4.4.5 The Performance & Risk Team record the results for each relevant performance indicator on the checklist for the month in question. Completion of the checklist produces a summary score for each performance indicator, which indicates how effectively officers have updated the information. 4.4.6 The Performance & Risk Team contact relevant officers regarding any issues identified during the monthly checks, in order to improve the quality of published data. The Performance & Risk Team also use the monthly checklists to identify common and persistent problems and escalate these issues to senior management if they remain unresolved. 4.5 Performance Indicator Procedure Notes 4.5.1 The Performance & Risk Team also had responsibility for one further entry that was ‘on target’ at the time of the last update report. This internal audit recommendation related to departmental procedure and guidance notes for performance indicators that the Council reports corporately – ‘A programme for the completion of procedure and guidance notes should be agreed and implemented. Notes should be reviewed annually or after significant change.’ 4.5.2 During early 2010, the Performance & Risk Team coordinated an organisation wide exercise to ensure that individual service areas produced procedure notes for all of their corporately reported performance indicators. This included providing service areas with partly completed templates and guidance notes relating to their full completion. 4.5.3 Following this exercise, individual service areas completed procedure notes for all relevant performance indicators. 4.5.4 The Performance & Risk Team continue to encourage and support service managers with the production and revision of procedure notes, although ultimately, it is the responsibility of individual service managers to ensure that procedure notes relating to their service area remain accurate and up to date. 4.6 National Indicator 35 4.6.1 One entry relating to National Indicator 35 (Building resilience to violent extremism), consisting of two internal audit recommendations, was ‘on target’ at the time of the last update report. The initial reasons behind the recommendations were that the Council received only one completed response from LSP members in 2008/09 and that subsequently the Council had not based its returns for NI35 on a representative sample of partner organisations. The Head of Policy, Partnerships & Community Development addressed these two recommendations for the 2009/10 returns, but this was in light of a changing approach to and an enhanced understanding of the indicator. AUDIT AND RISK (15.9.10) 4.6.2 The two audit recommendations are set out below, along with the Head of Policy, Partnerships & Community Development’s explanation of the changes implemented to address each one. 4.6.3. The internal audit recommended that the required templates should be issued sooner in the process (annually to tie in with the January/February LSP meeting) to allow partners more time to prepare their returns. 4.6.4 For 2009/10, the Council did not circulate the required templates to the whole LSP, as it had recently received confirmation from Special Branch, which monitors community and other tensions that North Hertfordshire remains a very low risk area. It is, therefore, important for the Council to equally manage the 'risk' of building fear of terrorism, and so the 2009/10 template was completed with information provided by the Hertfordshire Constabulary, NHDC Policy Team and our community partners who attended the December 2009 workshop. The template therefore represented a single, but partnership return, made with the assistance of faith and community groups regarding the local position, which was proportionate to local risk. 4.6.5 The second internal audit recommendation was that the engagement of LSP members should be actively sought during the year (within quarterly action plan reviews with the LSP and CDRP) in order to raise the profile and significance of this indicator, leading to an increased response rate for 2009/10. 4.6.6 The Council has included the 'prevent' initiative within the LSP work programme and has had several in-year presentations/reports recorded in the minutes for that partnership. This has raised the awareness of our partners, but it is also important that due to the reduced, very low risk of terrorism and alongside that managing the 'fear' that initial 'targeting' of specific community groups could have had in marginalising local communities, it has in place actions which conserve the current high levels of community cohesion. 86.5% of the local population feel this is an area in which people from different communities get on well together (1st place in Hertfordshire), so partners have agreed that a working group be established, to meet first in September 2010, not specifically to manage anti-terrorism, but to provide a continuing dialogue with all communities and retain that cohesion. 4.6.7 The Committee should be reassured that community 'tensions' continue to be monitored through community safety partnership work and that it is intended that a review of progress with the working group and NI35 itself, will form part of the work of the Partnership Scrutiny Sub Committee in the future. 4.6.8 The Head of Policy, Partnerships & Community Development deems that the NI35 entry is complete for the purpose of the improvement plan. 4.7 National Indicator 181 4.7.1 One improvement entry relating to National Indicator 181 (Average time taken to process HB/CTB new claims and change events), consisting of a single internal audit recommendation, was ‘on target’ at the time of the last update report. The recommendation was – ‘Data should be reported through Covalent when available.’ AUDIT AND RISK (15.9.10) 4.7.2 Since the last update report, the Department for Works and Pensions (DWP) has finally published performance data for this indicator. However, due to the difficulties previously experienced by the DWP in producing accurate data, the first year of data relates to the financial year 2009/10. 4.7.3 Data relating to the first three quarters of 2009/10 is now available on the Data Interchange Hub and the Performance & Risk Team has updated Covalent accordingly. The team has informed the Systems & Technical Manager of the update, in order that the published processing times can be compared with local management information, although NHDC is not able to replicate fully the DWP calculations. 01/04/09 – 30/06/09 12 calendar days 01/07/09 – 30/09/09 10 calendar days 01/10/09 – 31/12/09 4 calendar days 4.7.4 As previously reported to the Audit & Risk Sub Committee, the DWP is responsible for calculating and publishing data returns for NI181. Officers, therefore, can only update Covalent when the DWP makes data available. 4.7.5 However, Members should note that NHDC continues to submit the required data extracts to the DWP in a timely manner and is not contributing to any delays in publishing data. 4.7.6 Again, as previously reported, officers are still able to monitor the current processing times of new claims and change events without up to date NI181 data. Officers calculate this local management information using reports previously used to calculate best value performance indicators BV78a (speed of processing - new HB/CTB claims) and BV78b (speed of processing - changes of circumstances for HB/CTB claims). 4.7.7 The Performance & Risk Team will continue to monitor the publication of further NI181 performance data. 5. ISSUES RAISED AT THE AUDIT & RISK SUB-COMMITTEE MEETING ON 24TH FEBRUARY 5.1 Member Training 5.1.1 The Sub Committee requested that officers should consider the training needs of Members in relation to data quality and that an allowance should be made for this via e learning. 5.1.2 The initial training provided to officers concentrated on the production of performance data and the requirements of the NHDC Data Quality Policy. The Performance & Risk Team also provided further training to officers with specific responsibilities for entering and approving performance data on Covalent. 5.1.3 As Members are not actively involved in the production of performance data, the existing training is not specifically suited to Members. 5.1.4 However, Members use performance data to monitor service provision and to inform decision-making and therefore need to ensure that the data produced by officers is accurate and sufficient for its intended purpose. AUDIT AND RISK (15.9.10) 5.1.5 To assist, the Performance & Risk Team has produced a flowchart, which gives an overview of the submission process for corporate performance data and explains how officers apply their training in a working environment. The flowchart, is included as Appendix A to this report, and sets out the different stages and responsibilities throughout the process from start to finish. The Performance & Risk Team developed this process to identify problems and inaccuracies at the earliest opportunity and to ensure that performance data published on Covalent is always accurate and of the highest quality. 5.1.6 If the Committee feel that further training is still required, feedback on the specific requirements would be helpful to ensure that the appropriate training is made available. 5.2 Empty Properties Data 5.2.1 The last update report detailed a ‘completed’ improvement relating to the submission of empty properties data, as part of the HIP (Housing Investment Programme) HSSA (Housing Strategy Statistical Appendix) return to central government. 5.2.2 The Sub Committee requested confirmation that the improvement detailed in the report actually achieved the desired outcome of an accurate and timely submission of data. 5.2.3 The Housing Strategy & Renewals Manager worked closely with the Systems & Technical Manager to ensure that the 2009/10 data was in accordance with the HSSA guidance. Officers completed quality checks during June and early July and submitted the 2009/10 HIP HSSA return before the deadline date of the 23rd July 2010. 6. LEGAL IMPLICATIONS 6.1 There are no specific legal implications arising from this report. 7. FINANCIAL AND RISK IMPLICATIONS 7.1 There were no additional cost implications in completing the internal audit recommendations that formed the data quality improvement plan other than Officer time. 7.2 If data quality is not maintained then there is a risk that incorrect performance information is used by the Council which could lead to inappropriate actions /decisions being implemented. The actions taken by implementing this action plan will mitigate the risk of this occurring. 8. HUMAN RESOURCE AND EQUALITIES IMPLICATIONS 8.1 there are no direct human resource or equalities implications arising from this report. 9. CONSULTATION WITH EXTERNAL ORGANISATIONS AND WARD MEMBERS 9.1 Not applicable. AUDIT AND RISK (15.9.10) 10. RECOMMENDATIONS 10.1 That the Audit and Risk Committee note the completion of the actions that formed the Combined Data Quality Improvement Plan that was previously reported to the Audit & Risk Sub Committee. 11. REASONS FOR RECOMMENDATIONS 11.1 The internal and external audit recommendations that fed into the production of this Improvement Plan are now complete. 12. APPENDICES 12.1 Appendix A – overview of NHDC’s PI Data Submission Process 13. CONTACT OFFICERS 13.1 Fiona Timms Performance & Risk Manager 13.2 Tim Everitt Performance Improvement Officer 13.3 Andy Cavanagh Head of Finance, Performance & Asset Management 13.4 Tim Cowland Head of IT and Customer Services 13.5 Liz Green Head of Policy, Partnerships and Community Development 13.6 Mark Scanes Systems & Technical Manager 14. BACKGROUND PAPERS 14.1 Internal Audit reports on performance indicators 14.2 Combined Data Quality Improvement Plan AUDIT AND RISK (15.9.10)