ED-Guidelines-UTI-10_25_10
advertisement

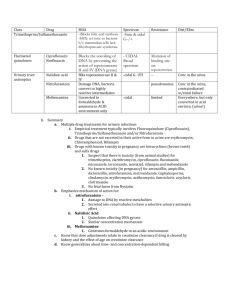
ED: Initial Empiric Antimicrobials for Urinary Tract Infections Condition Preferred treatment options Comments Trimethoprim-Sulfamethoxazole (TMP-SMX) 1 double-strength (DS) tablet (160 mg/800 mg) orally every 12 hours for 3 days 80-85% of acute uncomplicated cystitis cases are caused by E. coli followed by Staphylococcus saprophyticus. Uncomplicated Cystitis in Women If recently treated with a specific antibiotic class, would consider using an alternative class of antibiotic. If culture data available, tailor regimen to the appropriate antibiotic. OR 72% of community-acquired E. coli is susceptible to TMP-SMX. Cephalexin 250-500 mg every 6 Higher rates of susceptibility hours for 7 days seen in patients without history OR of antibiotic exposure (e.g., Ciprofloxacin 500 mg orally every young healthy women) 12 hours for 3 days Around 84% of E. coli is OR Nitrofurantoin (Macrobid®) 100 mg dose every 12 hours for 7 days susceptible to ciprofloxacin but resistance may be higher in the setting of recent fluoroquinolone use. Around 90% of outpatient E. coli isolates are susceptible to cephalexin. >95% of E. coli isolates are susceptible to nitrofurantoin. Nitrofurantoin is the most costly of these agents. In the case of prior Enterococcus infections consider using amoxicillin (500 mg three times a day for 7 days). *Please do not use moxifloxacin for urinary tract infections. Pyelonephritis in Women Outpatient therapy DO NOT USE NITROFURANTOIN FOR UPPER TRACT INFECTIONS Ciprofloxacin 500 mg orally every In the case of known 12 hours for 7- 14 days Enterococcus infections consider using amoxicillin or amoxicillinOR clavulanate. Cephalexin 500 mg every 6 hours for 10-14 days 10/25/10 *Please do not use moxifloxacin for urinary tract infections. OR TMP-SMX 1 DS tablet every 12 hours for 14 days Inpatient therapy Ceftriaxone 1-2 g IV every 24 hours OR Ceftriaxone has activity against 94% of E. coli isolates. It does not cover Enterococcus species. Ciprofloxacin 500 mg orally (or 400 mg IV) every 12 hours In the case of prior Enterococcus infections consider using ampicillin or ampicillinsulbactam. Cephalexin 250-500 mg orally every 6 hours for 7 days Fluoroquinolones should be avoided in pregnancy. OR Pregnant women should have a follow-up urine culture performed one to two weeks after treatment to ensure that bacteriuria has been eradicated. Pregnant Women Cystitis – treat as outpatients as long as they do not have symptoms suggestive of pyelonephritis Have a low threshold for hospitalization Acute pyelonephritis Nitrofurantoin (Macrobid®) 100 mg dose every 12 hours for 7 days Ceftriaxone 1-2 g IV every 24 hours for 10-14 days Men Urethritis, lower tract infection For men < 40 years old, consider STD testing and treatment ≥40 years old E. coli is the most common uropathogen DO NOT USE NITROFURANTOIN OR MOXIFLOXACIN Ciprofloxacin 500 mg orally every Urethritis should be strongly 12 hours for 7 days considered in sexually active men. Examination for penile OR ulcerations and urethral Trimethoprim-Sulfamethoxazole discharge and diagnostic tests (TMP-SMX) 1 double-strength for Neisseria gonorrhoeae and (DS) tablet (160 mg/800 mg) Chlamydia trachomatis are orally every 12 hours for 7 days warranted. Urinary DNA probe recommended please use appropriate kit (not swab). Acute pyelonephritis Ciprofloxacin 500 mg orally (or 400 mg IV) every 12 hours for 714 days OR 10/25/10 Any man presenting with pyelonephritis should have a complete urologic evaluation to determine causative factors. Trimethoprim-Sulfamethoxazole (TMP-SMX) 1 double-strength (DS) tablet (160 mg/800 mg) orally every 12 hours for 7-14 days Prostatitis Acute prostatitis can manifest as frequency, dysuria, and difficulty urinating with fever and a tender prostate on exam Ciprofloxacin 500 mg orally every In the presence of urinary 12 hours for 4 weeks retention or evidence of obstruction, please consult OR urology. Trimethoprim-Sulfamethoxazole Fluoroquinolone use in the (TMP-SMX) 1 double-strength elderly may lead to neurologic (DS) tablet (160 mg/800 mg) symptoms, patients and/or orally every 12 hours for 4-6 caregivers should be instructed weeks to monitor for signs and symptoms especially with prolonged courses. Healthcare-associated and/or catheter-associated Urinary Tract Infections Catheter-associated UTI patient being discharged from ER Remove catheter if not indicated. Use prior culture data to guide therapy. Patient should have signs and symptoms of a urinary tract infection (e.g., fever, chills, suprapubic tenderness, altered mental status) If catheter in place ≥ 2 weeks and remains indicated, it should be replaced. Obtain urinalysis and urinary culture from freshly placed catheter prior to initiation of antibiotics. Fluoroquinolone use in the elderly may lead to neurologic symptoms, patients and/or caregivers should be instructed to monitor for signs and symptoms especially with prolonged courses. DO NOT TREAT AYSYMPTOMATIC PYURIA OR BACTERIURIA If no prior exposure to fluoroquinolones, ciprofloxacin 500 mg orally every 12 hours for 7-14 days depending on symptom resolution. Alternatives include: Trimethoprim-Sulfamethoxazole (TMP-SMX) 1 double-strength (DS) tablet (160 mg/800 mg) orally every 12 hours for 7-14 days 10/25/10 Catheter-associated UTI, patient being admitted with no prior culture data Patient should have signs and symptoms of a urinary tract infection (e.g., fever, chills, suprapubic tenderness, altered mental status) DO NOT TREAT AYSYMPTOMATIC PYURIA OR BACTERIURIA Remove catheter if not indicated. Use prior culture data to guide therapy. If catheter in place ≥ 2 weeks and remains indicated, it should be replaced. Urinalysis and urinary culture obtained from freshly placed catheter prior to initiation of antibiotics. Ceftriaxone 1-2 g IV every 24 hours OR If severe β-lactam allergy: Ciprofloxacin 500 mg (400 mg IV) every 12 hours Healthcare-associated UTI patient with signs and symptoms of SIRS or urosepsis Please draw 2 sets of blood cultures Remove catheter if not indicated. Please use prior culture data to guide empiric therapy. If catheter in place ≥ 2 weeks and remains indicated, it should be replaced. Obtain urinalysis and urinary culture from freshly placed catheter prior to initiation of antibiotics. Cefepime 1-2 gram IV every 12 hours If severe β-lactam allergy: Aztreonam 1-2 grams IV every 812 hours Renal Transplant Recipient 1. N Engl J Med. 2003; 349: 259-66 2. Urology Clinic North Am. 2008; 5: 1-12 3. Am Fam Physician 2010; 81: 783-8 4. Clin Infect Dis. 2010; 50: 625-63 10/25/10 Please call Renal Transplant Service pager 5595 and/or Transplant ID 8678