Patient Health Questionnaire
advertisement

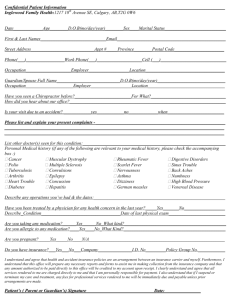
Patient Health Questionnaire Name: _________________________________________ Date of Birth: ______/_______/______ Do you have any medication allergies? ____ Yes ____ No If so, please list: ______________________________________________________________________________________________________________ ____________________________________________________________________________________________________________________________ Review of Systems: To the best of your knowledge, do you now have or have you ever had the following: Yes No CONSTITUTIONAL Curvature of the Spine Arthritis/Joint Pain Difficulty Walking Bruise Easily Psoriasis Eczema Liver Disease Stomach Ulcer PSYCHOLOGICAL Depression Drug/Alcohol Dependency Psychiatric Treatment ENDOCRINE Diabetes Thyroid Disorder HEMATOLOGIC/LYMPH Anemia Swollen Glands Immune Disease/AIDS Blood Clots Chronic Heartburn Pulmonary Emboli Unexplained Chills Unexplained Fever Significant Weight Gain Significant Weight Loss EYES Double Vision Vision Problems RESPIRATORY Asthma or Wheezing Shortness of Breath Chronic Cough Sleep Apnea GI TRACT Hiatal Hernia GENITAL/URINARY Urinary Tract Infection Kidney of Bladder Disease Difficulty Urinating NEUROLOGIC CARDIAC High Blood Pressure Heart Attack Irregular Heart Rate Pacemaker Rheumatic Fever No SKIN EAR/NOSE/THROAT Lack of Sense of Smell Hearing Loss Yes MUSCULAR/SKELETAL Polio Stroke Head Injury Numbness of Arm/Leg ALLERGY/IMMUNOLOGIC Iodine Shellfish Latex SOCIAL HISTORY Do you smoke? ____ Yes ____ No (Number of packs/day ____ for ____ years) Do you drink? ____ Yes ____ No (Number of drinks/week ____) Are you married ____ Yes ____ No Do you live alone? ____ Yes ____ No Level of Education: ____________________________________________________________________________________________________________ PAST HISTORY Any medical history not covered in previous questions? _______________________________________________________________________________ ____________________________________________________________________________________________________________________________ Are you pregnant or think you may be? ____ Yes ____ No Surgeries/Hospitalization Reason Year 1. __________________________________________________________________________________________________________________________ 2. __________________________________________________________________________________________________________________________ 3. __________________________________________________________________________________________________________________________ 4. __________________________________________________________________________________________________________________________ Medication that you are currently taking: Medication Dosage When you started taking 1. __________________________________________________________________________________________________________________________ 2. __________________________________________________________________________________________________________________________ 3. __________________________________________________________________________________________________________________________ 4. __________________________________________________________________________________________________________________________