Introduction
advertisement

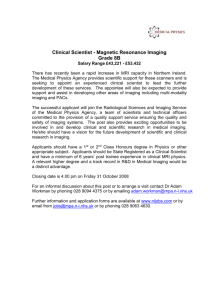
Molecular Imaging of Atherosclerosis Danny L. Costantini (1T3) Faculty of Medicine, University of Toronto and Department of Diagnostic Imaging, The Hospital for Sick Children, Toronto, ON, Canada Corresponding Author: Danny L. Costantini (1T3), MSc, PhD Corresponding Author’s Institution: The Hospital for Sick Children 555 University Ave Toronto, Ontario M5S 3M2 Tel: (416) 813-6029; FAX: (416) 813-7591 e-mail: dan.costantini@utoronto.ca Running Footline: Imaging of Atherosclerosis Abstract Molecular imaging is a rapidly evolving field that aims to develop novel technologies and methods to image specific biological processes in the living organism at the cellular and molecular level. This review discusses several novel nuclear medicinebased imaging strategies that exploit the unique biological properties of atherosclerosis to detect key aspects of the disease. Among the approaches, targeting macrophage activity, protease activity, apoptosis and angiogenesis for in vivo molecular imaging of atherosclerosis have demonstrated the greatest potential for translation into the clinical setting. Introduction Atherosclerosis is a systemic disease that affects most major arteries of the body and is the most common cause of premature death in the western world [1]. The disease occurs when high levels of cholesterol-containing low density lipoproteins (LDL) and other fatty materials in the blood accumulate within the arterial wall [2]. These fatty deposits recruit monocytes which move out of the bloodstream and into the endothelial wall where they become mature macrophages. Once resident, macrophages avidly ingest oxidized LDLs, cholesterol and other fatty materials via scavenger receptors, and transform into foam cells. In time, these fat-laden foam cells accumulate in the lining of the arterial wall and form fatty streaks that contribute to the expansion of a fibrous plaque. If the inflammatory process persists, the atherosclerotic plaque continues to evolve causing a gradual narrowing of the vessel lumen and thickening of the arterial wall [2]. Atherosclerosis remains clinically silent until the lesion expands to a point where it begins to limit blood flow causing symptoms of reversible ischemia during periods of high demand such as angina pectoris [3]. Alternatively, the fibrous plaque can erode and rupture, and produce thrombotic occlusions that can subsequently cause myocardial infarction or stroke. Unfortunately, most high-risk or “vulnerable plaques” are often unrecognized before causing these critical clinical events [3]. Indeed, rupture of the atherosclerotic plaque accounts for approximately 70% of fatal acute myocardial infarctions and/or sudden coronary deaths [4]. A number of non-invasive molecular imaging strategies have been proposed, therefore, to detect atherosclerotic plaques that are prone to become unstable and rupture. It is hoped that early detection of the vulnerable plaque will lead to more aggressive therapies to stabilize the plaque and prevent critical clinical events from occurring [5]. Imaging Modalities to Visualize the Atherosclerotic Plaque Many groups have focused on anatomic imaging modalities such as intravascular ultrasound, magnetic resonance imaging (MRI), or multi-slice computed tomography (CT) to view the vulnerable plaque [6-8]. Alternatively, nuclear imaging utilizes radiolabeled tracers (i.e. radiopharmaceuticals) which have properties that allow them to distribute differently in diseased tissues relative to normal ones. The radiopharmaceuticals are conjugated with gamma emitting radionuclides such as iodine-123 (123I), technetium-99m (99mTc), or indium-111 (111In) which permit their biodistribution to be visualized by external imaging [9]. A gamma scintillation camera, for example, is used to detect singlephoton emitting radionuclides such as 123 I, 99m Tc or 111 In. In planar imaging, the gamma camera remains stationary and the resulting images are in two-dimensions. Single photon emission computed tomography (SPECT) is similar to planar imaging, except that the resultant images are in three-dimensions because the gamma camera rotates around the patient. Standard transaxial images can be reconstructed from the collected data and can be re-oriented into coronal or sagittal slices. Alternatively, positron emission tomography (PET) scanning is based on the detection of two annihilation photons that originate from the decay of a positron-emitting radionuclide such as fluorine-18 (18F) or iodine-124 (124I). With the emission of photons at 180 degrees with respect to each other, 360 degree data acquisition can be performed. The principal advantage of PET is its greater temporal and spatial resolution and its greater sensitivity over standard gamma camera imaging [9]. The strength of nuclear imaging is its ability to provide quantitative physiological information on a functional level such as density of a specific receptor or the metabolic activity of a plaque. Moreover, the sensitivity of nuclear medicine is based on radiolabeled biomarkers with a signal sensitivity in the pico-molar range which is one million to one billion times above that of MRI or CT [4]. Since nuclear medicine-based imaging may be the most promising approach for vulnerable plaque detection, this review will focus primarily on this technology which currently is at a more advanced stage of development than other imaging modalities. 18F-FDG PET imaging for plaque inflammation Currently, the standard imaging technique for atherosclerosis is X-ray contrast angiography, which can identify the site and severity of luminal stenosis, but does not provide any information about plaque inflammation [1]. Clinically, this is important because anti-atheroma statin therapies can promote plaque stability by decreasing plaque macrophage content and activity without substantially reducing plaque size and thus, angiographic appearance [10]. Techniques that can quantify the inflammatory content of atherosclerotic plaques may therefore provide a better means to predict the risk of plaque rupture, and assess the effectiveness of anti-atheroma therapies [11]. There is mounting evidence to suggest that positron emission tomography (PET) with 18 F-fluorodeoxyglucose (18F-FDG) may be useful for imaging inflammation within atherosclerotic plaques [12]. 18 F-FDG is a PET radiotracer that competes with glucose for uptake into inflammatory cells such as activated macrophages that have high metabolic activity. Rudd et al [13], used 18 F-FDG to visualize plaque inflammation in patients with symptomatic carotid atherosclerosis. Eight patients who had experienced a recent carotid arterial ischemic event, and had an internal carotid artery lesion with >70% stenosis, received an intravenous injection of 18 F-FDG and underwent PET imaging 3 h later. Co- registration with subsequently acquired cranial computed tomography (CT) images demonstrated focal 18 F-FDG uptake in carotid plaques. The estimated accumulation of radiotracer in symptomatic lesions was approximately 27% higher than in contralateral asymptomatic lesions, and examination of surgically resected plaque specimens demonstrated heavy macrophage infiltration [13]. Thus, these findings demonstrate that 18 F-FDG PET could be useful in identifying inflamed carotid lesions. Several groups have argued that 18F-FDG-PET will prove less suitable for detecting coronary artery atherosclerosis due to the very high uptake of 18 F-FDG in metabolically active cardiomyocytes [1]. However, several case reports and retrospective studies have demonstrated anecdotal 18 F-FDG uptake in coronary arteries in oncologic patients (Fig.1) [14-17]. More recently [18], a prospective demonstrated the feasibility of precise 18 18 F-FDG PET study with multi-slice CT F-FDG localization within the coronary arties of patients presenting with acute coronary syndrome. In this study, the physiological uptake of 18 F-FDG by myocardium was almost entirely suppressed by administering a high-fat diet, which promoted instead the uptake of free fatty acids by the cardiomyocytes. Restricting carbohydrate meals 1 d before the study, and administering -blockers on the day of the study further minimized myocardial uptake of 18 F-FDG [12, 18]. By suppressing the normal uptake of 18F-FDG in cardiomyocytes, these investigators were able to localize the inflammatory regions within the coronary arties, as well as in some segments of the aortic root, thereby demonstrating that 18 F-FDG imaging of coronary inflammation is indeed feasible [12, 18]. Figure 1: Transaxial CT (A), 18F-FDG PET (B), and fused PET/CT (C) images. Focal 18FFDG uptake without significant calcifications is demonstrated in aortic arch from 72-y-old man with known ischemic heart disease and who underwent coronary artery bypass grafting 13 y previously, suggesting high level of inflammation activity within these plaques. Reprinted by permission of the Society of Nuclear Medicine from [15]. Imaging MMP activity in atherosclerotic plaques Macrophages, lymphocytes, vascular smooth muscle cells (SMCs) and vascular endothelial cells secrete a number of proteases such as matrix metalloproteinases (MMPs) that degrade the extracellular matrix (ECM) within the atherosclerotic plaque [19]. MMPs are a family of Zn2+-dependent endopeptidases comprising over 25 enzyme subtypes, including interstitial collagenases (MMP-1, -8, -13), gelatinases or basement membrane degrading MMPs (MMP-2, -9), stromelysins or matrilysins (MMP-3, -7), membrane-type MMPs (MMP-14 to -17), and others (MMP-12) [20]. MMPs play an important role in diverse physiologic processes such as organ development, angiogenesis and tissue repair. In vascular pathology, however, MMPs play a role in vascular remodeling, aneurysm formation, progression of atherosclerosis and plaque destabilization [21]. In human atherosclerotic plaques, an overexpression of the interstitial collagenases MMP-1, -8, and 13 and of gelatinase MMP-2 and -9 has been observed using immunohistological techniques [22-24]. Studies in animal models of atherosclerosis suggest that non-invasive imaging of MMP activity in vascular lesions is feasible, and can provide diagnostic information for evaluating the level of inflammation within a plaque. Hartung et al [21], for example, used the broad-spectrum MMP inhibitor (MPI) CGS-27023A, radiolabeled with 124 I (124I-MPI), to visualize MMP activity in atherosclerotic apolipoprotein E-deficient (ApoE-/-) mice. ApoE-/- mice were fed a cholesterol-rich diet and carotid plaques were induced in the animals by ligating the left common carotid artery. Coronal PET images through the left carotid lesion demonstrated intense uptake of the radiotracer in the lesion 30 min after intravenous administration (Fig. 2). The specific uptake in the carotid arteries was significantly higher in mice given the radioligand alone than in mice pretreated with an saturating amount of excess, unlabeled MPI [21]. These results were further confirmed by gamma counting of microsurgically excised common carotid arteries, which revealed a three-fold higher accumulation of radioactivity in the left common carotid (containing the lesion), compared to the right common carotid (control) [21]. Thus, these data suggest that MPI-scintigraphy may become a useful imaging method for non-invasive detection of MMP activity in the evaluation of atherosclerosis. Figure 2: Ex vivo dissection demonstrating the site of ligated left common carotid artery (left panel) and a corresponding high-resolution small animal PET scan (whole-body coronal slice - 0.4 mm thick) through a left carotid lesion (right panel) 4 weeks after ligation and a high calorie diet in an apoE−/− mouse. Intense uptake of the radiolabelled broad spectrum MMP inhibitor 124 I-MPI is seen in the left carotid lesion (arrow) 30 min after intravenous injection. Reproduced with permission from [21]. Annexin V imaging of apoptosis in atherosclerotic plaques Apoptosis or programmed cell death may contribute to atherosclerotic plaque vulnerability [25]. During the process of apoptosis, phosphatidylserine, a phospholipid normally residing on the inner cell membrane of viable cells, becomes externalized and thus available to bind affinity ligands such as annexin V [25]. Several scintigraphic imaging agents have been developed based on annexin V (e.g., 99mTc- and 123I-labeled annexin V for single photon mission CT [SPECT] imaging) [5]. Kolodgie et al [26], for example, demonstrated strong uptake of radiolabeled cholesterol-fed rabbits. 99m Tc-annexin V in balloon-injured aortas of 99m Tc-annexin V has also been used in a small pilot study for imaging of carotid atherosclerosis in patients with recent or remote cerebrovascular accidents [27]. Uptake of the radiotracer was reported only after recent cerebrovascular accidents and not seen in patients being treated with statins. Annexin V binding was localized to apoptotic macrophages and also to the red blood cell membranes embedded in necrotic cores. Radiolabeled annexin V thus provides another clinical option for imaging carotid atheroma. Higher resolution imaging agents using PET-compatible radiotracers such as 124 I- or 18 F-labeled annexin V may provide better avenues for coronary vascular imaging [12]. Molecular imaging of v3 integrin expression in atherosclerotic plaques The walls of coronary arteries are normally free of microvessels. In atherosclerotic plaques, however, there are dense networks of capillaries, referred to as vasa vasorum [28]. These microvessels grow when the wall thickness of the coronary artery exceeds the effective diffusion distance of oxygen. Atherosclerosis-induced angiogenesis is therefore of considerable clinical interest since plaque neovessels are thought to play a key role in the initiation and later rupture of plaques. Active endothelial cells within the atherosclerotic plaque characteristically overexpress the integrin v3, a cell adhesion molecule that mediates the migration of endothelial cells through the basement membrane [29]. Several radiolabeled v3 antagonists have demonstrated potential for imaging angiogenesis following myocardial or vascular injury. One particular study, for example, evaluated an 111 In-labeled quinolone (RP748) specific for v3 to image the angiogenic process in a canine model of myocardial infarction [30]. Dogs underwent coronary artery occlusion for two hours in order to stimulate angiogenesis in ischemic myocardium. At 3 weeks after reperfusion, ischemic regions of myocardium demonstrated an approximate four-fold increase in the uptake of 111 In-RP748 compared to normal myocardium. Hua et al [31], similarly evaluated a 99mTc-labeled peptide (NC100692) targeted at v3 in a murine model of hind-limb ischemia. At various times after surgical ligation of the right femoral artery, mice were intravenously administered the radiopharmaceutical and underwent planar gamma camera imaging. Planar images acquired at 3 and 7 days after femoral ligation demonstrated significantly higher radioactivity in the ischemic hind-limb compared with the contralateral nonischemic hind-limb. Moreover, gamma well counting demonstrated a three-fold greater retention of radioactivity in ischemic muscle compared with the contralateral nonischemic muscle. These preliminary studies suggest that radiolabeled compounds targeting v3 integrin may be valuable noninvasive markers of angiogenesis after ischemic injury. Additional studies will be required, however, to validate the applicability of this imaging strategy to detect angiogenesis induced by atherosclerosis. Conclusion The biology of atherosclerosis provides several potential biomarkers for plaque imaging such as MMPs, annexin V, and angiogenesis integrins. Among the approaches, 18 F-FDG is the most investigated tracer, but the discovery of other biological markers associated with atherosclerotic disease may show promise for plaque detection [12, 19, 32]. Despite primary and secondary prevention strategies, atherosclerotic vascular diseases continue to be one of the leading causes of death worldwide [5]. The promising pre-clinical and clinical findings described above could have a significant impact on our ability to visualize atherosclerosis in its early stages, and to monitor the effectiveness of atheromamodifying therapies throughout the course of treatment. However, the efficacy of these novel imaging technologies will have to be assessed in appropriately designed prospective clinical trials before these discoveries can be successfully translated into a clinically useful imaging test to visualize the vulnerable plaque. References [1] Davies JR, Rudd JH, Weissberg PL: Molecular and metabolic imaging of atherosclerosis. J Nucl Med 2004; 45(11): 1898-907. [2] Berliner JA, Navab M, Fogelman AM, et al.: Atherosclerosis: basic mechanisms. Oxidation, inflammation, and genetics. Circulation 1995; 91(9): 2488-96. [3] Jang IK: Can angiographically silent coronary atherosclerosis predict mortality after cardiac transplantation? Nat Clin Pract Cardiovasc Med 2005; 2(8): 386-7. [4] Langer HF, Haubner R, Pichler BJ, Gawaz M: Radionuclide imaging: a molecular key to the atherosclerotic plaque. J Am Coll Cardiol 2008; 52(1): 1-12. [5] Jaffer FA, Libby P, Weissleder R: Molecular and cellular imaging of atherosclerosis: emerging applications. J Am Coll Cardiol 2006; 47(7): 1328-38. [6] Nissen SE, Yock P: Intravascular ultrasound: novel pathophysiological insights and current clinical applications. Circulation 2001; 103(4): 604-16. [7] Schmermund A, Erbel R: Unstable coronary plaque and its relation to coronary calcium. Circulation 2001; 104(14): 1682-7. [8] Schroeder S, Kopp AF, Baumbach A, et al.: Noninvasive detection and evaluation of atherosclerotic coronary plaques with multislice computed tomography. J Am Coll Cardiol 2001; 37(5): 1430-5. [9] Wilson AM: Textbook of Nuclear Medicine. Philadelphia: Lippincott-Raven Publishers, 1998. [10] Crisby M, Nordin-Fredriksson G, Shah PK, Yano J, Zhu J, Nilsson J: Pravastatin treatment increases collagen content and decreases lipid content, inflammation, metalloproteinases, and cell death in human carotid plaques: implications for plaque stabilization. Circulation 2001; 103(7): 926-33. [11] Jaffer FA, Libby P, Weissleder R: Molecular imaging of cardiovascular disease. Circulation 2007; 116(9): 1052-61. [12] Tahara N, Imaizumi T, Virmani R, Narula J: Clinical feasibility of molecular imaging of plaque inflammation in atherosclerosis. J Nucl Med 2009; 50(3): 331-4. [13] Rudd JH, Warburton EA, Fryer TD, et al.: Imaging atherosclerotic plaque inflammation with [18F]-fluorodeoxyglucose positron emission tomography. Circulation 2002; 105(23): 2708-11. [14] Alexanderson E, Slomka P, Cheng V, et al.: Fusion of positron emission tomography and coronary computed tomographic angiography identifies fluorine 18 fluorodeoxyglucose uptake in the left main coronary artery soft plaque. J Nucl Cardiol 2008; 15(6): 841-3. [15] Ben-Haim S, Kupzov E, Tamir A, Israel O: Evaluation of 18F-FDG uptake and arterial wall calcifications using 18F-FDG PET/CT. J Nucl Med 2004; 45(11): 1816-21. [16] Paulmier B, Duet M, Khayat R, et al.: Arterial wall uptake of fluorodeoxyglucose on PET imaging in stable cancer disease patients indicates higher risk for cardiovascular events. J Nucl Cardiol 2008; 15(2): 209-17. [17] Rominger A, Saam T, Wolpers S, et al.: 18F-FDG PET/CT identifies patients at risk for future vascular events in an otherwise asymptomatic cohort with neoplastic disease. J Nucl Med 2009; 50(10): 1611-20. [18] Rogers IS, Figueroa AL, K N: Assessment of coronary segment inflammation with combined 18-fluorodeoxyglucose positron emission tomography and 64-slice multidetector computed tomography [abstract]. Circulation 2007; 2007(116(suppl II)): 410. [19] Jaffer FA, Weissleder R: Seeing within: molecular imaging of the cardiovascular system. Circ Res 2004; 94(4): 433-45. [20] Rudek MA, Venitz J, Figg WD: Matrix metalloproteinase inhibitors: do they have a place in anticancer therapy? Pharmacotherapy 2002; 22(6): 705-20. [21] Hartung D, Schafers M, Fujimoto S, et al.: Targeting of matrix metalloproteinase activation for noninvasive detection of vulnerable atherosclerotic lesions. Eur J Nucl Med Mol Imaging 2007; 34 Suppl 1: S1-8. [22] Sukhova GK, Schonbeck U, Rabkin E, et al.: Evidence for increased collagenolysis by interstitial collagenases-1 and -3 in vulnerable human atheromatous plaques. Circulation 1999; 99(19): 2503-9. [23] Herman MP, Sukhova GK, Libby P, et al.: Expression of neutrophil collagenase (matrix metalloproteinase-8) in human atheroma: a novel collagenolytic pathway suggested by transcriptional profiling. Circulation 2001; 104(16): 1899-904. [24] Galis ZS, Sukhova GK, Lark MW, Libby P: Increased expression of matrix metalloproteinases and matrix degrading activity in vulnerable regions of human atherosclerotic plaques. J Clin Invest 1994; 94(6): 2493-503. [25] Geng YJ, Libby P: Progression of atheroma: a struggle between death and procreation. Arterioscler Thromb Vasc Biol 2002; 22(9): 1370-80. [26] Kolodgie FD, Petrov A, Virmani R, et al.: Targeting of apoptotic macrophages and experimental atheroma with radiolabeled annexin V: a technique with potential for noninvasive imaging of vulnerable plaque. Circulation 2003; 108(25): 3134-9. [27] Kietselaer BL, Reutelingsperger CP, Heidendal GA, et al.: Noninvasive detection of plaque instability with use of radiolabeled annexin A5 in patients with carotid-artery atherosclerosis. N Engl J Med 2004; 350(14): 1472-3. [28] Herrmann J, Lerman LO, Mukhopadhyay D, Napoli C, Lerman A: Angiogenesis in atherogenesis. Arterioscler Thromb Vasc Biol 2006; 26(9): 1948-57. [29] Westlin WF: Integrins as targets of angiogenesis inhibition. Cancer J 2001; 7 Suppl 3: S139-43. [30] Meoli DF, Sadeghi MM, Krassilnikova S, et al.: Noninvasive imaging of myocardial angiogenesis following experimental myocardial infarction. J Clin Invest 2004; 113(12): 1684-91. [31] Hua J, Dobrucki LW, Sadeghi MM, et al.: Noninvasive imaging of angiogenesis with a 99mTc-labeled peptide targeted at alphavbeta3 integrin after murine hindlimb ischemia. Circulation 2005; 111(24): 3255-60. [32] Liu Y, Abendschein D, Woodard GE, et al.: Molecular Imaging of Atherosclerotic Plaque with 64Cu-Labeled Natriuretic Peptide and PET. J Nucl Med 2009.