confined space risk assessment form
advertisement

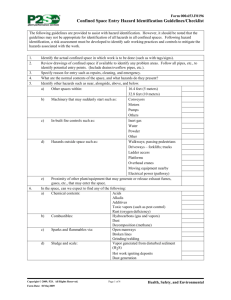
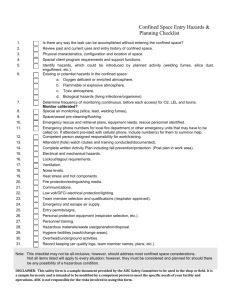
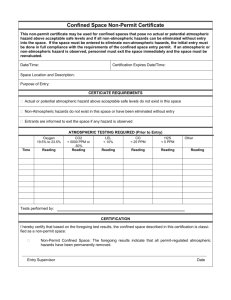
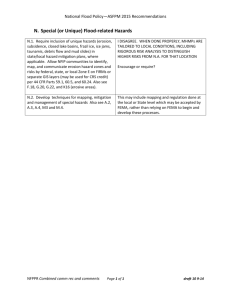
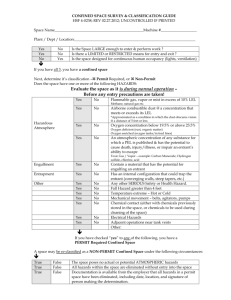
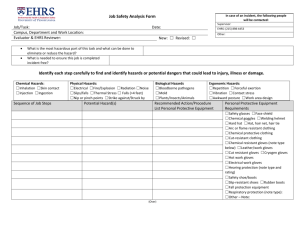
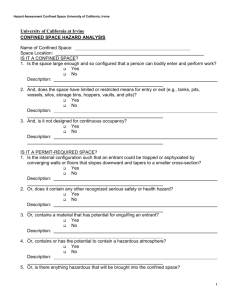
Employer’s Name 4.8.2 Confined Space Safety Risk Assessment Form CONFINED SPACE RISK ASSESSMENT FORM CONFINED SPACE RISK ASSESSMENT Risk Assessment Conducted By: Date of Assessment: Confined Space Location: Time of Assessment: / / AM/PM Description of Plant: Description of Work: Identification if a confined spaces Yes No Potential hazards 1. Is the space enclosed or partially enclosed? 2. It the space not designed or intended to be occupied by a person? Is the space designed or intended to be at normal atmospheric pressure while a person is in the space?? Is the atmosphere in the confined space a concern? 1. Can machinery start while in the space? 2. Is the space likely to pose a risk to health and safety from: Can entanglement with machinery occur? an atmosphere that does not have a safe oxygen level? Can liquid or steam flow (inrush) while in the space? 3. contaminants including airborne gases, vapour and dusts? Is isolation a concern? Harmful concentrations of any airborne contaminants? Uncontrolled introduction of substances? Engulfment? Biological Hazards Mechanical Hazards Potential hazards Yes No Electrical Hazards? Restricted entry or exit? Skin contact with hazardous substances? Harmful airborne contaminants? Noise? May have oxygen levels below 19.5%? Manual Tasks? Oxygen may be in excess? Radiation? May have hydrogen sulphide present? Environmental? Fire and Explosion? Hazards outside confined space? Engiulfment? Other? Is the work area a confined space? Yes Gases carbon monoxide, carbon dioxide, methane gas present? Note: A risk assessment MUST be completed for any YES answers (turn page to complete). NOTE: Please maintain a copy of this record sheet. No Compiled: 10/2012 Revision No: 1 – Employer’s Name Confined Space Safety Risk Assessment Form CONFINED SPACE RISK ASSESSMENT Description of Hazard / Risk from any ‘Yes’ answers on the previous page 1. 3. 2. 4. RISK ASSESSMENT CONTROLS OPTIONS YES NO ELIMINATE – Can the process be eliminated completely? SUBSTITUTE – Can the process be replaced with a safer one? If YES, Detail Action: Hazard 1 ISOLATE – Can the process or person be isolated from risk? If YES, Detail Action: Hazard 2 ENGINEER – Can the process be re-designed? If YES, tick the options to be used: Indicate the risk assessment consequences and likelihood in the columns below. (Example Consequence – Major Likelihood – Unlikely – Risk Score H Consequence Likelihood Risk Score Natural Ventilation Hazards / Risks Associated Blower Fan Hazard 3 ADMINISTRATION – Can we limit exposure to the risk by: job rotation work procedure training Hazard 4 PPE – Can we use Personal Protective Equipment? Code: E – Extreme Risk, H – High Risk, M – Moderate risk, L – Low risk No. Risk Level Prior to Control Control Measures / Corrective Action Risk Level After Control Implemented Yes / No Verification Corrective Action has been taken. Competent Person Name: Competent Person Signature: Date: Supervisor Name: Supervisor Signature: Date: NOTE: Please maintain a copy of this record sheet. / / Compiled: 10/2012 Revision No: 1 – / /