Supplemental Methods Biomarker Analysis Venous blood was
advertisement

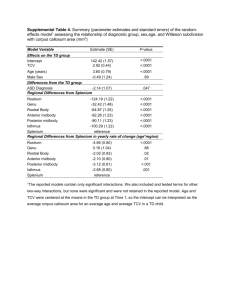
Supplemental Methods Biomarker Analysis Venous blood was collected in tubes containing EDTA and was maintained at 40 C for 4 hours or less. Plasma was then removed and frozen at -800 C until assays were performed. High sensitivity C-reactive protein (hs-CRP) was analyzed on thawed samples by the Roche/Hitachi 912 System, Tina-quant assay (Roche Diagnostics, Indianapolis, IN). The detection range of this assay was 0.1 mg/liter to 20 mg/liter. Values above the upper limit were designated as 20 mg/liter.(1) Cystatin-C was analyzed by a BNII nephelometer (Dade Behring, Inc, Deerfield, Ill; now Siemens Healthcare Diagnostics, Inc) with a particle enhanced immunonephelometric assay (N Latex Cystatin C, Dade Behring, Inc). Monoclonal antibodies coated on polystyrene particles that agglutinate were used to magnify the amount of scattered light based on cystatin-C concentrations. The detection range of this assay was 0.195 mg/L to 7.330 mg/L.(2) NT-pro-BNP was analyzed by Elecsys pro-BNP platform (Roche Diagnostics, Indianapolis, Indiana).(3) Adiponectin level was measured by a commercial sandwich enzymelinked immunosorbent assay (Millipore, Billerica, MA, USA).(4) Leptin was analyzed by a commercially available radioimmunoassay (Linco Research Inc., St. Charles, Missouri). The lowest detectable level was 0.5 μg/L, and all lower values were designated as 0.5 μg/L.(5) IL-6 concentrations were determined using a Luminex sandwich assay with a detection range between 10-15,000 pg/mL. Homeostatic model assessment-insulin resistance (HOMA-IR) was calculated from fasting glucose and insulin levels using the following formula: fasting plasma insulin x fasting plasma glucose / 22.5.(6) References (1) Khera A, Vega GL, Das SR et al. Sex differences in the relationship between C-reactive protein and body fat. J Clin Endocrinol Metab 2009;94:3251-8. (2) Patel PC, Ayers CR, Murphy SA et al. Association of cystatin C with left ventricular structure and function: the Dallas Heart Study. Circulation Heart failure 2009;2:98-104. (3) Das SR, Abdullah SM, Leonard D et al. Association between renal function and circulating levels of natriuretic peptides (from the Dallas Heart Study). The American journal of cardiology 2008;102:1394-8. (4) Turer AT, Khera A, Ayers CR et al. Adipose tissue mass and location affect circulating adiponectin levels. Diabetologia 2011;54:2515-24. (5) Abdullah SM, Khera A, Leonard D et al. Sex differences in the association between leptin and CRP: results from the Dallas Heart Study. Atherosclerosis 2007;195:404-10. (6) Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care 2004;27:1487-95. Supplemental Methods Statistical Analysis Variance inflation factors and correlations coefficients of the adipose tissue and anthropomorphic variables used in the multivariate model. (a) Spearman correlation matrix of BMI and adiposity measures: RP fat BMI IP fat VAT SAT RP fat BMI 0.57 p<.0001 IP fat 0.84 p<.0001 0.63 p<.0001 VAT 0.93 p<.0001 0.63 0.98 p<.0001 p<.0001 SAT 0.43 p<.0001 0.86 0.52 p<.0001 p<.0001 0.51 p<.0001 LBF 0.13 p=0.0001 0.67 0.21 p<.0001 p<.0001 0.19 0.81 p<.0001 p<.0001 (b) Variance inflation factors from the full model Adiposity Measure VIF BMI 6.8 RP fat 1.7 IP fat 2.1 SAT 5.9 Liver fat 1.4 LBF 4.8 LBF Supplemental Figure 1:Forest plot demonstrating that the relative risk (95% CI) of VAT on the development of hypertension is independent of circulating markers of renal function (cystatin-C), inflammatory markers (hs-CRP, IL-6), adipocytokines (leptin, adiponectin), insulin-resistance (HOMA-IR) or NT-pro-BNP. Supplemental Figure 2: An increased incidence of hypertension was noted across sex- and race-specific tertiles of (a) VAT or (b) RP even among those participants among the lowest baseline sex- and race-specific quartile of SAT.