Personal information is strictly for the use of Student/University
advertisement

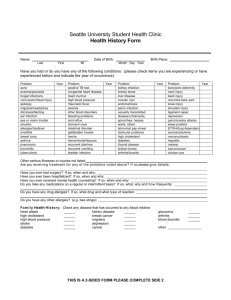
Personal information is strictly for the use of Student/University Health Services and will not be released to anyone without your knowledge or consent. ETSU STUDENT/UNIVERSITY HEALTH SERVICES Please Print Legibly in INK Social Security Number ___ ___ ___-___ ___-___ ___ ___ ___ PO BOX 70675 Johnson City, TN 37614 Form will not be processed without this number REPORT OF MEDICAL HISTORY ETSU ID# E____________________ ___ PLEASE COMPLETE THIS FORM AND BRING WITH YOU FOR YOUR APPOINTMENT! SEX: M FIRST NAME MIDDLE LAST NAME HOME ADDRESS (NUMBER AND STREET) CITY STATE ZIP CODE DATE OF BIRTH NAME, RELATIONSHIP, AND ADDRESS OF EMERGENCY CONTACT (BUSINESS) MARITAL STATUS: SINGLE MARRIED WIDOWED OTHER AGE (HOME) PHONE NUMBER DO YOU HAVE INSURANCE? YES NO Have any of your grandparents, parents or siblings ever had any of the following diagnosed illnesses? Immediate Family History: STATE OF HEALTH F AGE OF DEATH OCCUPATION CAUSE OF DEATH YES FATHER TUBERCULOSIS MOTHER DIABETES NO RELATIONSHIP KIDNEY DISEASE BROTHERS HEART DISEASE ARTHRITIS STOMACH DISEASE ASTHMA SISTERS MIGRAINE EPILEPSY, CONVULSIONS CANCER (what type) THYROID DISEASE PERSONAL HISTORY Please answer all Questions. Comment on all positive answers in space provided or on back of this sheet. YES ALLERGIES TO MEDICATIONS (DESCRIBE ALL REACTIONS) NO COMMENTS: Additional medication allergies and description of allergic response: PENICILLIN SULFONAMIDES SERUM OTHER ALLERGIES TO FOODS A. Has your physical activity been restricted during the last five years due to a chronic condition? (Give reason and durations) B. Have you been exposed to violence in the home, school or community? C. Have you received treatment or counseling for a nervous condition, personality or character disorder, or emotional problem? D. Have you had any chronic illnesses or injuries or been hospitalized other than already noted? (Give Details) E. Have you consulted or been treated by clinics, physicians, healers, or other practitioners within the past five years? (Other than for routine checkups) List food allergies PERSONAL HISTORY, CONTINUED YES NO COMMENTS: F. Have you been rejected for or discharged from military service because of physical, emotional, or other reasons? If yes, give reasons. G. List Date of last pap, Date of Last Vision Exam, Date of Last Dental Exam. PERSONAL HISTORY: Have you been diagnosed with any of the following illnesses? HAVE YOU HAD? YES NO YES NO YES NO YES Rheumatic Fever Worry or Nervousness Heart Murmur Dizziness, Fainting Scarlet Fever Frequent Anxiety High/Low Blood Pressure Weakness, Paralysis Chicken Pox Frequent Depression Palpitations (heart) MALES ONLY: Measles Insomnia Disease/Injury of Joints Testicular Pain /Swelling Mumps Recurrent Headache Arthritis Penile Discharge German Measles Recurrent Colds Ear, Nose, Throat Trouble Genital Warts Malaria Head Injury with Unconsciousness Back Problems Painful Urination Gum or Tooth Trouble Hay Fever/Asthma Tumor, Cyst FEMALES ONLY: Sinusitis Tuberculosis Stomach /Intestinal Trouble Abnormal Pap Eye Trouble Shortness of Breath Cancer Irregular Periods Epilepsy, Convulsions Chronic Cough Jaundice Severe Cramps Surgery: Rupture Hernia Sexually Transmitted Diseases Excessive Flow Appendectomy Migraine Headaches Urinary Tract Infections or kidney problems/disease Vaginal Infections Tonsillectomy Diabetes Gallbladder Trouble or Gallstones Genital Warts Hernia Repair Low Blood Sugar Recurrent Diarrhea Ovarian Cysts or Tumors Other Surgery Known heart problems Recent Gain or Loss of Weight Other Vein Problems, Blood Clots Pain/Pressure in Chest “Trick” knee, Shoulder, etc.” Other Comments: Patient’s Signature: Date: Reviewed by: Date: NO