Medical History Form
advertisement

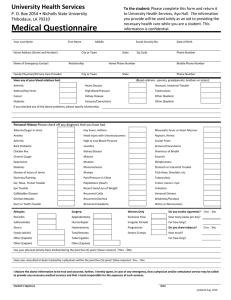
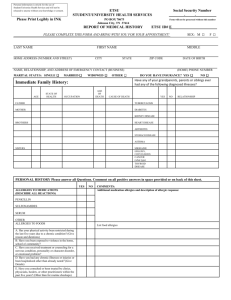
MEDICAL HISTORY Vinson Health Center LAST NAME (PRINT) FIRST MIDDLE SOCIAL SECURTY NUMBER (OR) MUSTANGS ID NUMBER LOCAL ADDRESS (NUMBER AND STREET) CITY STATE LOCAL CELL PHONE NUMBER LOCAL PHONE NUMBER ZIP CODE DATE OF BIRTH SEX/ETHNICITY YOUR PREFERRED EMAIL ADDRESS IN CASE OF EMERGENCY (USA ONLY) RELATIONSHIP IN CASE OF EMERGENCY ADDRESS (NUMBER, STREET, APT.) CITY HOME/CELL NUMBER (USA ONLY) STATE ZIP CODE Have any of your relatives ever had any of the following? Yes No Relationship Yes Tuberculosis Arthritis Diabetes Stomach Disease Asthma, Hay Fever Epilepsy, Convulsions Kidney Disease Heart Disease No Relationship Personal History (PLEASE ANSWER ALL QUESTIONS) Comment on all positive answers in the space below or attach additional page Have you had? Yes No Have you had? Yes No Have you had? Yes No Have you had? Scarlet fever Frequent anxiety Chronic cough Venereal disease Measles Frequent depression Palpitations (heart) Albumin/Sugar in urine German measles Worry or Nervousness High or Low Blood Pressure Frequent Urination Mumps Recurrent Headache Rheumatic Fever or Heart Murmur Female Only Chicken Pox Recurrent Colds Disease or Injury of Joints Irregular Periods Malaria Trick Knee, Shoulder, etc. Sever Cramps Gum or tooth trouble Head Injury with Unconsciousness Hay Fever, Asthma Back Problems Excessive Flow Tuberculosis Sinusitis Tumor, Cancer, Cyst Diabetes Ear, eye, nose, throat trouble Surgery Shortness of Breath Pain/Pressure in Chest Jaundice Stomach or Intestinal Trouble Are you Allergic to: Gallbladder Trouble or Gallstones Appendectomy Penicillin Recurrent Diarrhea Tonsillectomy Hernia Repair Sulfonamides Serum Rupture, Hernia Recent Gain or Loss of Weight Other Foods (which) Dizziness, Fainting Insomnia Other No Yes No Comments: Weakness, Paralysis Yes No A.Has your physical activity been restricted during the past five years? C.Do you take any prescription medication? If so, please list. B.Have you received treatment or counseling for a nervous condiction, personality or character disorder, or emotional problem? (Give Details) D.Have you had any illness or injury or been hospitalized other than already noted? (Give Details) I acknowledge that the above information is correct. Signed_______________________________________________________Date___________________________________ 7/15 Yes Report of Medical History Vinson Health Center To provide you with the best possible health care at the Vinson Health Center, we ask that you complete this Medical History report. The information you furnish on the Medical History form is for use by the Vinson Health Center and will not be released to anyone without your knowledge and consent. Senate Bill 157 requires certain immunizations for specific classes of students. If you are enrolling in Health Related courses, you must furnish proof of immunization. Patient Rights I have read and/or received a copy of my “Patient Rights” (Initial) __________ Notice of Privacy Practices I have read and/or received a copy of the “Notice of Privacy Practices” (Initial) __________ Advanced Directive (Living Will) Do you have an Advanced Directive or Living Will? If YES, please provide a copy for our records. Y_____ For All Students: By signing below, I verify that the information provided on this form is correct. _____________________ DATE Return to: Vinson Health Center Midwestern State University 3410 Taft Blvd. Wichita Falls, Texas 76308-2099 _______________________________________ STUDENT SIGNATURE (Please Complete Both Sides) N_____