2015 - Hennepin County
advertisement

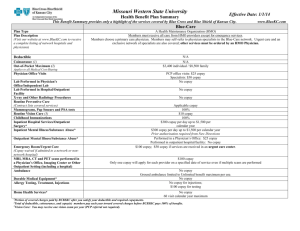
2015 Health Summary of Benefits with Health Incentive Standard (Administered by PreferredOne) No Copay at the Be Well Clinic for covered adults All other HCMC clinics subject to regular office visit copay Tier 1 Deductibles and Out of Pocket Lifetime maximum Calendar year deductible None Calendar year out of pocket maximum Preventive Health Care Routine physical, eye exams, immunizations Prenatal and postnatal care Office Visits Illness or injury Allergy injections Physical, speech and occupational therapy Chiropractic care Mental health care / substance abuse Emergency Care Urgent Care Center Emergency care at a hospital ER Ambulance Inpatient Hospital Care Illness or injury Mental health / substance abuse Outpatient Care Scheduled outpatient (non surgical) Scheduled outpatient surgeries Outpatient MRI and CT Durable Medical Equipment (DME) DME and prosthetic devices Retail Pharmacy (up to 30 day supply) Generic drug Brand name drug Mail Order Pharmacy ( up to a 90 day supply) Generic drug Brand name drug Tier 2 Tier 3 Unlimited $50 Single; $75 Single; $500 per covered person; $100 Family $150 Family $1500 per family $2500 per person; $4500 per family 100% coverage $15 copay $15 copay $15 copay $0 copay $30 copay Out of Network $20 copay 100% coverage $20 copay $20 copay $20 copay 70% coverage after deductible $35 copay $35 copay $35 copay $20 copay $35 copay $100 copay 80% coverage 70% coverage after deductible 75% coverage after deductible $125 copay $135 copay $260 copay 70% coverage after deductible $15 copay $50 copay $20 copay $60 copay 80% coverage $35 copay $110 copay 70% coverage after deductible 80% coverage 70% coverage after deductible $15 copay $40 copay 70% coverage after deductible $30 copay $80 copay 70% coverage after deductible This is only a summary; for additional details and complete benefit information see the complete Summary of Benefits (member contract). 7/2/2015 2015 Health Summary of Benefits with Health Incentive Advantage (Administered by PreferredOne) Fairview - North Memorial - HealthEast FIRST 3 OFFICE VISITS, URGENT CARE OR E VISITS PER MEMBER PER YEAR - NO COPAY (highlighted below) No Copay at the Be Well Clinic for covered adults In Network Deductibles and Out of Pocket Lifetime maximum Calendar year deductible Calendar year out of pocket maximum Preventive Health Care Routine physical, eye exams, immunizations Prenatal and postnatal care Office Visits Illness or injury Allergy injections Physical, speech and occupational therapy Chiropractic care Mental health care / substance abuse Emergency Care Urgent Care Center Emergency care at a hospital ER Ambulance Out of Network Unlimited $500 per covered person; None $1500 per family $2500 per person; $4500 per family 100% coverage 70% coverage after deductible $15 copay 100% coverage $15 copay $15 copay $0 copay 70% coverage after deductible $15 copay 75% coverage after deductible $100 copay 80% coverage $125 copay 70% coverage after deductible Outpatient Care Scheduled outpatient (non surgical) Scheduled outpatient surgeries Outpatient MRI and CT $15 copay $50 copay 80% coverage 70% coverage after deductible Durable Medical Equipment (DME) DME and prosthetic devices 80% coverage 70% coverage after deductible $15 copay $40 copay 70% coverage after deductible $30 copay $80 copay 70% coverage after deductible Inpatient Hospital Care Illness or injury Mental health / substance abuse Retail Pharmacy (up to 30 day supply) Generic drug Brand name drug Mail Order Pharmacy ( up to a 90 day supply) Generic drug Brand name drug This is only a summary; for additional details and complete benefit information see the complete Summary of Benefits (member contract). 7/2/2015 2015 Health Summary of Benefits with Health Incentive Advantage (Administered by PreferredOne) HealthPartners - Park Nicollet FIRST 3 OFFICE VISITS, URGENT CARE OR E VISITS PER MEMBER PER YEAR - NO COPAY (highlighted below) No Copay at the Be Well Clinic for covered adults In Network Deductibles and Out of Pocket Lifetime maximum Calendar year deductible Calendar year out of pocket maximum Preventive Health Care Routine physical, eye exams, immunizations Prenatal and postnatal care Office Visits Illness or injury Allergy injections Physical, speech and occupational therapy Chiropractic care Mental health care / substance abuse Emergency Care Urgent Care Center Emergency care at a hospital ER Ambulance Out of Network Unlimited $500 per covered person; None $1500 per family $2500 per person; $4500 per family 100% coverage 70% coverage after deductible $15 copay 100% coverage $15 copay $15 copay $0 copay 70% coverage after deductible $15 copay 75% coverage after deductible $100 copay 80% coverage $125 copay 70% coverage after deductible Outpatient Care Scheduled outpatient (non surgical) Scheduled outpatient surgeries Outpatient MRI and CT $15 copay $50 copay 80% coverage 70% coverage after deductible Durable Medical Equipment (DME) DME and prosthetic devices 80% coverage 70% coverage after deductible $15 copay $40 copay 70% coverage after deductible $30 copay $80 copay 70% coverage after deductible Inpatient Hospital Care Illness or injury Mental health / substance abuse Retail Pharmacy (up to 30 day supply) Generic drug Brand name drug Mail Order Pharmacy ( up to a 90 day supply) Generic drug Brand name drug This is only a summary; for additional details and complete benefit information see the complete Summary of Benefits (member contract). 7/2/2015 2015 Health Summary of Benefits with Health Incentive Advantage (Administered by PreferredOne) Hennepin County Medical Center - NorthPoint FIRST 3 OFFICE VISITS, URGENT CARE OR E VISITS PER MEMBER PER YEAR - NO COPAY (highlighted below) No Copay at the Be Well Clinic for covered adults HCMC or NorthPoint providers All other in-network providers Deductibles and Out of Pocket Lifetime maximum Out of Network Unlimited $500 per covered person; $1500 per family $2500 per person; $4500 per family Calendar year deductible None Calendar year out of pocket maximum Preventive Health Care Routine physical, eye exams, immunizations Prenatal and postnatal care Office Visits Illness or injury Allergy injections Physical, speech and occupational therapy Chiropractic care Mental health care / substance abuse Emergency Care Urgent Care Center Emergency care at a hospital ER Ambulance 100% coverage $0 copay 70% coverage after deductible $15 copay 100% coverage $0 copay $0 copay $15 copay $15 copay 70% coverage after deductible $15 copay $100 copay 80% coverage 75% coverage after deductible $0 copay $0 copay Inpatient Hospital Care Illness or injury Mental health / substance abuse $125 copay Outpatient Care Scheduled outpatient (non surgical) Scheduled outpatient surgeries Outpatient MRI and CT Durable Medical Equipment (DME) DME and prosthetic devices Retail Pharmacy (up to 30 day supply) Generic drug Brand name drug Mail Order Pharmacy ( up to a 90 day supply) Generic drug Brand name drug $0 copay $0 copay 70% coverage after deductible $15 copay $50 copay 70% coverage after deductible 80% coverage 80% coverage 70% coverage after deductible $15 copay $40 copay 70% coverage after deductible $30 copay $80 copay 70% coverage after deductible This is only a summary; for additional details and complete benefit information see the complete Summary of Benefits (member contract). 7/2/2015