Leukopenia Mgmt - ETCprotocols.org
advertisement

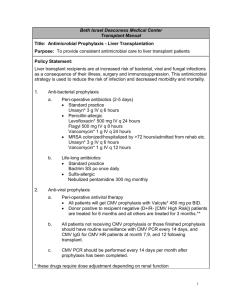
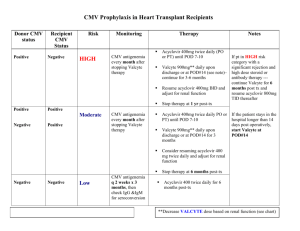
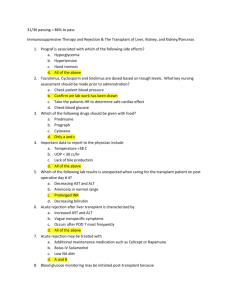
Policy: Kidney/Pancreas Post Transplant: Leukopenia Policy Statement: Activation Date: 05.01.2015 Affected Departments: Emory University Hospital’s Kidney (Pancreas) Transplant Programs Vision Strategy: Patient Care Protocol Statement: These guidelines are to be used by Emory Kidney (Pancreas) Transplant team clinicians for the management of leukopenia post kidney (pancreas) transplantation. Scope/Procedure: Basis: Leukopenia is a common occurrence after renal transplantation and in many cases results from immunosuppressive medications and/or viral infections. The underlying etiology of the leukopenia may be: 1. Medications 2. Immunosuppressive agents: mycofenolate mofetil (MMF or Cellcept), mycophenolic acid (Myfortic), azathioprine, sirolimus, Thymoglobulin 3. Antiinfective agents: valganciclovir, ganciclovir, trimetoprim-sulfametoxazole, penicillins. 4. Infections: CMV, or any viral infection. 5. Hypersplenism, especially in liver-kidney transplant recipients. General Guidelines: The general approach to the management of leukopenia is as follows: 1. Evaluate concomitant medications, especially thymoglobulin, mycophenolate, sirolimus, or azathioprine. 2. For all WBC <3,000, check differential 3. Rule out CMV viremia. 4. For ANC <1000: a) If on valganciclovir 900mg daily (or renally adjusted equivalent) for CMV prophylaxis, reduce dose by 50% b) If on valganciclovir 450mg daily (or renally adjusted equivalent) for CMV prophylaxis, hold valganciclovir and check weekly CMV PCRs for remainder of prophylaxis period or until ANC recovery and valganciclovir restarted. Restart prophylaxis once ANC > 1,000 c) Reduce mycophenolate dose by 25% d) Consider filgrastrim if clinically indicated e) Repeat CBC with differential weekly until ANC >1,000 f) For ANC <750 or no response to above interventions: g) Reduce mycophenolate by 50% (or additional 25%) h) Repeat CBC with differential in 1-4 days i) Discuss with provider based on clinical course/response j) Consider filgrastrim if clinically indicated 5. For ANC <500 or no response to above interventions: a) Hold mycophenolate (depending on clinical course) b) Administer filgrastrim c) Repeat CBC with differential every 1 – 4 days d) If ANC <500 and patient febrile (>38 C): Admit to hospital and start broad spectrum antibiotic coverage. 6. Reintroduce and/or increase mycophenolate dose when leukopenia corrected. References: Medical Care of the Kidney Transplant Recipient after the First Posttransplant Year. Djamali et al. Clin J Am Soc Nephrol 1: 623-640, 2006 Approved by: Renal Transplant Leadership Group Approval Date: 05/21/2008, 10/22/2008, 4/29/2015 Review Date: 12/09/2009 Regulatory References: Related Policies/Procedures: Approved By Renal Transplant Leadership Group