Clinical Outcomes of a Pediatric Safety Surveillance Program
advertisement

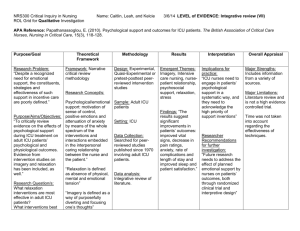
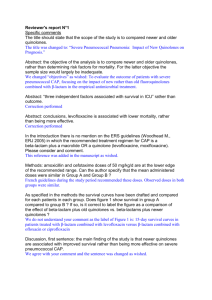
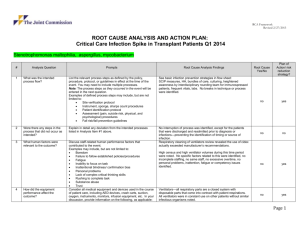
Clinical Outcomes of a Pediatric Safety Surveillance Program Murchie, W.E., Roberts, J.S., Leininger, R.J., Clifton, H., Smith, S. Seattle Children’s Hospital, Seattle, WA Background: A safety surveillance program was created to provide proactive acuity surveillance and critical care expertise for acute care patients and to reduce severe clinical deteriorations resulting in transfer to the intensive care unit (ICU) and resuscitation. Methods: A Recognized Illness Severity in Kids (RISK) nurse role was implemented in March 2013. The RISK nurse is a dedicated 24/7 ICU nurse who proactively meets with acute care staff, monitors acute care, and is the nurse responder for rapid response team calls. Their focus was early identification of patients at risk for clinical deterioration using a modified pediatric early warning score and clinical triggers thus facilitating prompt nursing and medical intervention. Training included parent perspectives, didactic courses, and simulation. A Transfer Requiring Intensive Care Practice (TRIP) was used to define a clinical change in a patient’s status which required both transfer to the ICU and resuscitation (non-invasive positive pressure ventilation, intubation, or vasoactive support) within two hours. This facilitated prompt nursing and provider intervention to prevent TRIP’s. TRIP rate, ICU average length of stay (ALOS), and 28 day mortality was compared pre-program implementation (2012) and post-program implementation (2014). Results: Between 2012 and 2014, the TRIP event rate decreased from 1.78 per 1000 non-ICU patient days to 1.1 per 1000 non-ICU patient days. ICU ALOS for patients meeting TRIP criteria decreased from 10.61 days to 7.88 days, while non-TRIP events ICU ALOS decreased from 7.21 days to 4.71 days. Twenty eight day mortality for patients meeting TRIP criteria decreased from 14.3% to 6%. Non-TRIP event 28 day mortality decreased from 4% to 3.4%. In 2012 rapid response calls totaled 455. Rapid response calls increased to a total of 708, a 55.6% increase, in 2014. The ICU transfer rates for our RRT calls increased from 33.5 % to 55.2%. Conclusions: Substantial reductions in TRIP events, ICU ALOS, and 28 day mortality were seen after implementing a pediatric safety surveillance program. In addition, increased safety surveillance was associated with an increase in RRT calls and ICU transfer rate. The authors have no conflicts of interest to disclose. Wendy Murchie, MN, RN, CCRN Joan Roberts, MD Wendy.murchie@seattlechildrens.org Joan.roberts@seattlechildrens.org