Form
advertisement

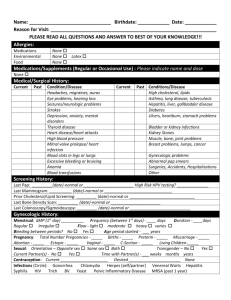
Current Medical Status Name:____________________________________________________ Date:__________________________ Review of Systems Are you bothered at the present time or during the last year by any of the following: Constitutional Fatigue Dizziness Problems with general health Recent weight loss Recent weight gain Y N __ __ __ __ Eyes Decreased vision Loss of vision Discharge Double vision Eye pain Y __ __ __ __ __ N __ __ __ __ __ ENT, Mouth Sore throat Hoarse voice Hearing loss Tinnitus Sinus problems Ear pain Y __ __ __ __ __ __ N __ __ __ __ __ __ Cardiovascular Chest pain Shortness of breath Palpitations Y __ __ __ N __ __ __ Respiratory Chronic/freq cough Coughing/ spitting up blood Wheezing Shortness of breath Y N __ __ Neurological Dizziness Fainting spells Loss of consciousness Frequent headaches Migraines Difficulty speaking __ __ __ __ __ __ __ __ __ __ __ __ Y __ __ __ __ __ __ N __ __ __ __ __ __ Difficulty moving or walking Tremors Abnormal numbness or sensation Seizures __ __ __ __ __ __ __ __ Gastrointestinal Difficult/painful swallowing Heartburn Nausea Vomiting Indigestion Hemorrhoids Rectal bleeding Black tarry stools Constipation Diarrhea Change in bowel habits Abdominal pain Y N __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ Genitourinary For women: Irregular or abnormally heavy periods Vaginal discharge Vaginal bleeding Burning with urination Blood in urine Excessive urination Menopause Y N __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ __ For men: Poor urine stream Prostate trouble Erection difficulty Burning with urination Blood in urine Excessive urination __ __ __ __ __ __ __ __ __ __ __ __ Musculoskeletal Neck pain Back pain Muscle spasms Decreased range of motion Joint/bone pain Weakness Y __ __ __ N __ __ __ Skin Rashes Skin lesion Ulcers Itching Eczema Skin problems Y __ __ __ __ __ __ N __ __ __ __ __ __ Psychiatric Anxiety Depression Mood swings Insomnia Y __ __ __ __ N __ __ __ __ Endocrine Heat intolerance Cold intolerance Fatigue Excessive thirst Excessive urination Y __ __ __ __ __ N __ __ __ __ __ Hematologic/Lymph Enlarged lymph nodes Fever Bruising Bleeding tendencies Neck lumps Y N __ __ __ __ __ __ __ __ __ __ Allergic/ImmunologicY Hives __ Recurrent infections __ Hay fever __ N __ __ __ __ __ __ __ __ __ List any other problems, including any change in your health status or surgery in the past 12 months: _________________________________________________________________________________________________________ _________________________________________________________________________________________________________ Have you ever smoked? Y N If Yes… Age started? _______ # years smoked? _______ # packs per day? _______ Why did you quit? _________________________________________________________________________________________ Name:_____________________________________ Do you drink alcohol? Y N If Yes… Liquor: #_____ per day/week/month (circle one) Beer: #_____per day/week/month Wine: #_____per day/week/month Do you drink caffeine? Y N If Yes… Tea Soda Coffee Allergies or adverse reaction to medications? Y N #_____ cups per day #_____ cups per day #_____ cups per day List: _______________________________________________________ ____________________________________________________________________________________________________________ Current occupation: ___________________________________________________________________________________________ Describe current exercise: ______________________________________________________________________________________ ____________________________________________________________________________________________________________ Describe current diet: __________________________________________________________________________________________ ____________________________________________________________________________________________________________ List current medications, including prescription, non-prescription, vitamins, supplements and herbs, as well as dose and frequency: ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ ____________________________________________________________________________________________________________ The following questions about personal habits are important in regard to your risk for a variety of medical problems: Do you wear seat belts? Y N Do you wear a bike helmet? Y N Is there a gun in your home? Y N If Yes… Are there children in the home? Y N Is the gun unloaded? Y N Have you ever engaged in any activity which has put you at risk of getting AIDS? Y N Do you wish to be tested for AIDS? Y N Have you ever worked with any of the following: Chemicals? Paints? Asbestos? Hazardous materials? Y Y Y Y N N N N Are you in a relationship in which you have been physically hurt (e.g. slapped, kicked, punched, bruised) by your partner? Y N Do you ever feel afraid of your partner? Y N Do you have a "living will"? Y N Do you have donor card? Y N