Renal Lab 2: Tubules, Interstitium and Vessels (March 25 or 26)
advertisement
")
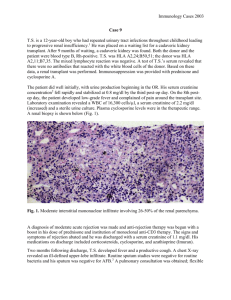
Renal Lab 1: Tubules, Interstitium, Vessels Case 1: (Answer: Acute tubular necrosis following severe intravascular volume depletion) A 54-year-old man (82kg) presents to the E.R. with malaise, fatigue and oliguria two days after serving on a pit-crew during the Indianapolis 500 race. Despite sunny skies and temperatures that hovered in the 90’s, he wore a full-body, fire-proof insulated suit and helmet so the he could change tires for a car that placed 28th out of 33 cars. He drank three 24-ounce bottles of purified water (2.1 liters) over eight or nine hours that day. He appears pale and his heart rate is 90/min, BP 108/60 mmHg, temperature 99.8F but he has no other physical findings. A stat serum creatinine = 5.8mg/dL, BUN = 70 mg/dL and hematocrit = 49%. You admit the patient and observe that over the next eight hours he has made only 60cc of urine and his serum creatinine is now 6.3 mg/dL. Questions: A) What is the most likely reason for decreased urine output? ischemia from intravascular volume depletion and subsequent decreased renal blood flow and tubular damage. (Renal tubules are damaged as a consequence of effective ischemia.) B) What problems is this patient having because of poor urine output? Hyperkalemia, acidosis, volume overload including pulmonary edema. C) What other laboratory values would you want to know? Potassium (hyperkalemia) and bicarb (acidosis). D) What therapy might be necessary? renal replacement therapy (dialysis) E) What would you expect the renal biopsy to show? 1. Light micro: normal glomeruli & vessels. Tubules would show changes of ATN: patchy (focal) loss of apical brush borders, blebbing of cytoplasm into lumina, hyaline casts &/or granular material in lumina (can occlude lumen); mitotic figures and flattened/squamoid cytoplasm (regenerating epithelial carpet); sometimes may see rupture of TBM (tubulorrhexis = bad). The most susceptible are the straight portion of the proximal tubule and the thick ascending limb. Make sure there are no crescents (RPGN). Interstitium may contain inflammatory cells as a reaction to the ATN (not a primary event in interstitium). 2. IF and EM – exclusion of glomerular causes, but not helpful in diagnosis of ATN (glomeruli should be negative or normal) G) Why is radiocontrast a bad idea in this patient? Contrast is not a good idea in a patient with ATN (exacerbates pre-existing acute injury). Case 2: (Answer: Acute cellular rejection in transplant recipient) A 48-year-old postal worker (60 kg female) presents to you three months after receiving a livingrelated renal allograft for chronic kidney disease secondary to autosomal dominant polycystic kidney disease. The patient's last serum creatinine two weeks ago was 1.2 mg/dl. Laboratory results from this visit reveal a serum creatinine of 1.9 mg/dl and a cyclosporine level of 400 ug/l by monoclonal RIA (elevated). On the exam the patient has a blood pressure of 160/95 mmHg and she is slightly tender over her graft sight. She started back to work this week. Questions: A) What is the differential diagnosis associated with this acute clinical presentation? List differential diagnoses under categories of pre-renal, renal and post-renal. B) How can you clinically distinguish between the categories of pre-renal, renal and post-renal?? 1. Pre-renal: history consistent with orthostasis, newly prescribed diuretics, GI loss or decreased fluid intake, fever, etc.; exam findings for intravascular volume depletion/hypovolemia, e.g. orthostasis, poor skin turgor 2. Renal: history of transplant; new meds; systemic or multisystem illness; negative exam. 3. Post-renal: history - symptoms of prostatism; abdom surgeries, etc; exam: suprapubic tenderness/bladder distension C) If you suspect that cyclosporine A is the cause of acute renal failure, how is the diagnosis made? How would you treat the patient? Either clinically by history or changing dosage and/or levels, or by biopsy. Treat by decreasing the dosage of offending drug. D) When is it appropriate to biopsy the patient and what might the renal biopsy show? Diagnosis: Acute cellular rejection: normal glomeruli and vessels, tubulitis (lymphocytes in tubule wall) which is graded according to Banff criteria (important for students to know there is a grading system that directs therapy). Contrast to cyclosporine toxicity with isometric vacuolization of proximal tubule cell cytoplasm, stripe-fibrosis in the interstitium and transmural hyalin deposition in small vessels (interlobular arteries and smaller). IF and EM are not helpful at this stage (would likely be normal/negative and thereby exclude other causes) Case 3: (Answer: Interstitial nephritis secondary to antibiotics) An 18-year-old female presents with complaints of a diffuse rash. Ten days ago the patient was prescribed cephalexin for a lower extremity cellulitis that developed after scratching a mosquito bite. She states the cellulitis improved but yesterday when a rash appeared on her chest and legs she started taking ibuprofen. On exam the patient has a temperature of 101.5 F and a diffuse erythematous maculopapular rash. Her serum creatinine is 2.5 mg/dl and differential white blood cell count reveals 10% eosinophils (absolute count 1000). Questions: A) What would you expect to see on urinalysis? WBC's (mostly lymphocytes and some neutrophils and eosinophils but these are hard to differentiate in the urine; IU Hospital no longer does Hensels because of low sensitivity and specificity, Wright’s stain is considered low yield by the IU clinical pathology lab). Also may detect low-grade proteinuria, and maybe WBC casts on urine microscopy. B) What other laboratory tests would you order? This is a classic presentation of acute intersitial nephritis secondary to an antibiotic. No other tests are necessary. C) How would you manage the patient? Is a renal biopsy necessary? Stop the antibiotic. Would expect patient to start to recover renal function within about a week. Creatinine might continue to rise until then and patient might be oliguric. If renal function is not improving by 1 week, consider doing a renal biopsy. If diagnosis confirmed, consider steroids as therapy. D) What would the renal biopsy show? 1. Light microscopy: glomeruli and vessels normal. Interstitium is edematous and contains infiltrate of lymphocytes (major cell component), macrophages, plasma cells, eosinophils and occasional neutrophils (PMNs should be minor, if present in the majority and/or in tubule lumina, the patient might have acute pyelonephritis). Tubules are generally normal although if interstitial nephritis is pronounced, might see changes that look like ATN). 2. IF and EM – does not contribute to diagnosis (other than to exclude glomerulonephritis, as glomeruli should be negative/normal by IF and EM) **************************************** Case 4: (Answer: Thrombotic microangiopathy c/w malignant hypertension) A 40-year-old man (70 kg) presents with complaints of headache that has increased in severity over the last several days and has been associated with blurred vision over the last 12 hours. On exam he has a blood pressure of 230/135 mmHg and an S4 gallop on auscultation of the heart. Urine dipstick detected blood and protein. Questions: A) You refer the patient to the ER where your fellow intern sees this patient. What would be important signs to elicit on physical exam? Fundoscopic exam (retinal hemmorhages, exudates, papilledema), abdominal bruit, multiple ectopy or tachycardia, crackles or tachypnea (pulmonary edema), asymmetric pulses suggesting dissection of aorta. B) What laboratory tests would you order? BUN & Creatinine to check renal function. Urine microscopy to check for RBCs and RBC casts (casts confirming glomerulus as origin of hematuria). C) What treatment would you immediately begin? Lower BP with intravenous drugs slowly to 160/90 mmHg range. Monitor for signs of organ ischemia (mental status changes, angina, decreasing urine output). D) The next morning, with excellent management, the BP is 156/92 mmHg and serum creatinine is 2.9 mg/dL. What would you do next? Put patient on oral meds and wean the intravenous drugs keeping blood pressure in the 140-160/90-100 mmHg range and slowly bringing BP down to <130/80 mmHg over several days. E) When is a kidney biopsy indicated? Biopsy only if proteinuria and hematuria persist (i.e., other underlying causes of glomerular disease) or if serum creatinine continues to climb over the next few days. What would the biopsy show? (Slides on web at “ANGEL”) 1. Light Microscopy: A. Vessels show: a. fibrinoid necrosis (eosinophilic, smudged material, may react with anti-fibrin antibodies) b. onionskin change (hyperplastic arteriolitis): concentric layers of proliferating intimal smooth muscle cells c. mucinous (myxoid) degeneration: loose, blue material in the vessel wall. d. fragmented RBCs in “lumina” B. Glomerular lesions are characterized by ischemic alterations (wrinkled GBM), hemorrhage, thrombosis and fibrinoid necrosis. If the patient’s malignant hypertension is superimposed on pre-existing benign hypertension, the vessels may contain hyaline deposits (chronic) along with fibrin (acute). “Hyaline” is PAS-positive (glassy-pink on H&E) and defined as nonspecific accumulation of plasma proteins and lipids. 2. IF: +/- detect fibrin (IgG, IgA, IgM, C3, C4, C1q usu. weak to negative/noncontributory). 3. EM would show widened subendothelium with granular, flocculent material along inner aspect of GBM. Electron dense (immune-type) deposits are usually absent. F) The patient is scheduled for follow-up with his primary care physician in one week. What other studies would be appropriate as an outpatient? If patient does not have history of longstanding severe hypertension or a family history, work up for secondary causes of hypertension, such as renal artery stenosis, would be appropriate.