DI-Chest-Solitary nodule
advertisement

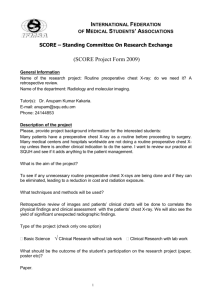
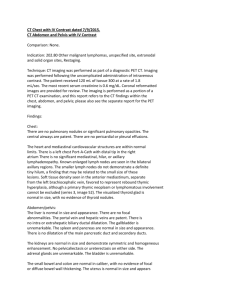
RADIOLOGY CASE REPORT Patient ID: OH# 22625693 Date of Study: July 21st, 2008 Type of Study: Chest X-ray (CXR) Clinical Indication: ID: 31 year old female HPI: Pt presented with chest pain of 2 months duration PMHx; Previous history of breast cancer. Pt had a left mastectomy and left axillary node dissection. In addition, the Pt had resection of part of the left anterior chest wall with mesh graft reconstruction. There has also been a partial resection in the superior segment of the right lower lobe of a previous metastatic lesion. Picture: Describe the radiological findings: PA: Solitary nodule located in right upper mid hemithorax. Approximately 1.5 cm in diameter. Moderately heterogeneous and rounded. Lateral: Solitary nodule located in posterior hemithorax adjacent to the chest wall. Appearance of smooth sloped edges sliding on to the chest wall (i.e. the appearance of a snow ball thrown against the wall). A solitary pulmonary nodule is defined as a single discrete pulmonary opacity that is surrounded by normal lung tissue and is not associated with adenopathy or atelectasis. Radiographically, a nodule is defined as a lesion smaller than 3 cm. Anything larger than 3 cm is termed a mass. Provide possible diagnosis(es): Neoplasm: Benign or malignant - Benign neoplasms such as hamartomas, lipomas, and fibromas - Malignant: Bronchogenic carcinoma - Small cell, large cell, adenocarcinoma, and squamous Carcinoids Solitary metastases Granuloma: Tuberculosis, histoplasmosis Infection: Round pneumonia, bacterial abscess Vascular: Infarct, Wegener’s granulomatosis, Rheumatoid arthritis Considering the Pt has a previous history of cancer, there is a higher likelihood that this nodule represents a new malignancy or metastatic lesion. Given the “snowball thrown against the wall” appearance of the opacity adjacent to the chest wall, this opacity may represent metastatic involvement of the lung pleura. What would you recommend next for this patient? - - It is important to first obtain prior radiographs to determine if this nodule is new or if the nodule has grown. Secondly, a CT thorax with IV contrast should be performed. This would aid in determining an accurate location and description of the nodule. Morphologic features of specific diagnosis are better visualized (eg, rounded atelectasis, arteriovenous malformations). It would also allow for characterization of soft tissue or bony involvement such as adjacent destruction of the muscle/ ribs or involvement of the pleura. Multiple nodules can be detected on CT scans as well as staging of malignancy. An ultrasound guided or CT-guided transthoracic fine needle aspiration should be performed for pathological diagnosis. A CT of the abdomen and pelvis with IV contrast should be performed to determine if any other lesions (i.e. metastases) have occurred. Is the use of this test/procedure appropriate? With a previous history of breast cancer and new onset chest pain, a CXR is a very good first screening test to determine if any new lesions have occurred in the chest. The CXR will also help rule out other causes of chest pain including lung infections, cardiac causes or even chest wall abnormalities. As mentioned above, a patient with prior history of cancer is at increased risk of metastases and thus further imaging with CT scans of at least the thorax, abdomen and pelvis would be necessary. Is (are) there any alternate test(s)? As mentioned above, an alternate test would be a CT thorax with IV contrast. This isn’t really an alternate in this case though as it should be performed to better characterize the lesion and aid in management. How would you explain to the patient about the possible risks and benefits of this test? Benefits of CXR CXR is fast (approx 15 min) and non invasive No radiation remains in a patient's body after an x-ray examination X-rays usually have no side effects Risks of CXR There is always a slight chance of cancer from radiation. However, the benefit of an accurate diagnosis far outweighs the risk The chest x-ray is one of the lowest radiation exposure medical examinations performed today. The effective radiation dose from this procedure is about 0.1 mSv, which is about the same as the average person receives from background radiation in 10 days Women should always inform their physician or x-ray technologist if there is any possibility that they are pregnant Benefits of CT scan CT scanning is painless, noninvasive and accurate A major advantage of CT is that it is able to image bone, soft tissue and blood vessels all at the same time Unlike conventional x-rays, CT scanning provides very detailed images of many types of tissue as well as the lungs, bones, and blood vessels CT examinations are fast and simple CT imaging provides real-time imaging, making it a good tool for guiding minimally invasive procedures such as needle biopsies and needle aspirations of many areas of the body, particularly the lungs, abdomen, pelvis and bones A diagnosis determined by CT scanning may eliminate the need for exploratory surgery and surgical biopsy No radiation remains in a patient's body after a CT examination X-rays used in CT scans usually have no side effects Risk of CT scan There is always a slight chance of cancer from radiation. However, the benefit of an accurate diagnosis far outweighs the risk The effective radiation dose from this procedure is about 10 mSv, which is about the same as the average person receives from background radiation in three years CT scanning is, in general, not recommended for pregnant women because of potential risk to the baby Nursing mothers should wait for 24 hours after contrast material injection before resuming breastfeeding The risk of serious allergic reaction to contrast materials that contain iodine is rare, and radiology departments are well-equipped to deal with them There is also a risk of contrast induced nephropathy most commonly defined as acute renal failure occurring within 48 hours of exposure to intravascular radiographic contrast material. Appropriate renal function testing including creatinine levels or creatinine clearance is required in patients with known renal disease 8. What is the cost of this test? The approximate cost of a CXR is $ 40.00-60.00. A CT scan with IV contrast of the abdomen and pelvis costs approximately $ 2000.00. However there is a wide range of costs for CT scans.