病历 case histroy
2011.3.8
• 一般事项 date of admission /marital status
/present address /correspondence /
occupation
• 主诉 chief complaints
现病史 present illness / history of present
illness
既往史 past medical history
家族史 family history
个人病史 personal history / social history
曾用药物 medications
过敏史 allergies
系统回顾 system review / review of system
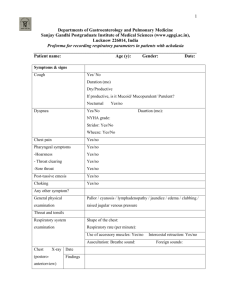
体检 physical examination
• 一般状况或全身状况 general appearance
头眼与耳鼻喉 head,eyes,ear,nose,throat
• 胸部与心肺 CHEST,heart,and lungs
腹部 abdomens
四肢extremities
神经系统nervous system,Neurological
• 骨骼肌系统 Musculoskeletal
泌尿生殖系统 Genitourinary
化验室资料 laboratorydata
血液检查 blood test
化学7项指标 chem.-7
心脑电图 electrocardiogram /
electroencephalogram , 略作 EKG/EEG
X线检查 X-ray examination, x-ray slides
• CT 扫描 computerized x-ray tomography
• 其他检查资料 other lab data
• 印象与诊断 impression and diagnosis
住院治疗情况 hospital course
出院医嘱 discharge instructions /
recommendations
出院后用药 discharge medications
Medical Records for Admission
• General information
•
Name: Huahua
• Age: three
• Sex: Female
• Race: Han
• Nationality: China
• Address: NO.23, Xicheng Road, Lucheng District, Wenzhou,
•
•
•
•
•
•
Zhejiang. Tel: 85763723
Parents Name: father Zhang Hesheng
Mother Yang Chiulian
Date of admission: September 18th, 2009
Date of record: 11Am, May 8th, 2001
Complainer of history: patient’s mother
Reliability: Reliable
• Chief complaint:
sore throat
for 48 h,.respiratory distress for
12h.
Present illness
• .A previously healthy 3-year-old girl was brought
to our emergency room in severe respiratory
distress. She had a sore throat for the past 48 h,
mild fever and minor respiratory difficulty
without cough.
•
Since onset, her appetite was not good, and
both her spiritedness and physical energy are bad.
Defecation and urination are normal.
Past history
Past medical history was significant for
prematurity (35 weeks’ gestation)
and transient tachypnoea.
Physical examination
•
Vital signs included: temperature 38.2°C, blood
pressure 75/40 mm Hg, heart rate 185 beats/min
and respiratory rate 60breaths/min.
• The patient was in a critical condition with a
diminished level of consciousness. She showed
tachypnoea, laboured and abdominal breathing,
nasal flaring, perioral cyanosis and pale skin.
Hypoventilation and rales were also present.
Crepitus was palpable over the neck and upper
chest.
Investigation
• Arterial blood PO2 was 58 mm Hg,
PCO2 34 mm Hg and oxygenation 70%
with an inspired oxygen
• fraction (FiO2) of 50%. White blood
cell count was normal.
• C-reactive protein and procalcitonin
were elevated
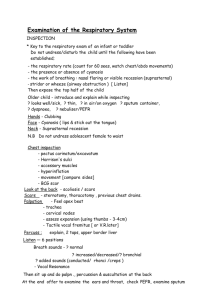
Chest radiograph
The initial chest
radiograph showed
pneumomediastinum with
subcutaneous emphysema,
right pneumothorax,
bilateral increased lung
density and left lower
lobe air bronchogram.
Hospital Course
• The patient was intubated and transferred
to the intensive care unit (ICU). A chest
tube was placed for pneumothorax
drainage.
• Despite supportive measures and reexpansion of the right lung, the patient’s
condition deteriorated in the following 36
h. A chest CT scan was obtained in order
to evaluate extension and complications of
the disease.
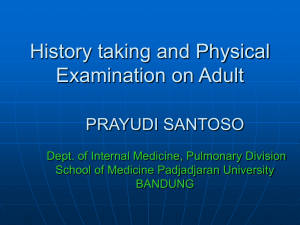
CT
• This revealed a sizeable
pneumomediastinum with
subcutaneous air, areas of
ground-glass attenuation and
air-space consolidation involving the entire lung
parenchyma, bilateral small
pleural effusions and residual
air in the right pleural space.
There were no bullae.
QUESTION?
1.What is the most likely diagnosis?
differential diagnosis?
2.Which examination should we do ?
3.How to treat this patient?