Case study #1

Unit 3 - Case Study #1
Admitting History
A 43-year-old woman was admitted to the hospital for an exploratory thoracotomy to diagnose and excise a 1.5-cm pulmonary nodule that had resisted diagnosis by bronchoscopy and percutaneous needle biopsy. She has been a registered nurse for the past 15 years and, up until about a year ago, was the director of nursing at the admitting hospital. For the past 4 months, she has been working the night shift as a general floor nurse in a nursing home owned by the hospital. Over the past 3 years, she has rapidly moved from a normal, healthy weight to obesity.
Over the last 6 months, she almost always has worn one of the same three outfits and increased her smoking from one to two-and-a-half packs of cigarettes a day. Her general hygiene has been poor, and her hair often appears dirty. Her estranged husband reported that she has been depressed for the past year or so. He disclosed that he suggested that they both see a marriage counselor, to no avail. Frustrated, he moved into his brother’s apartment a few miles away from his wife. Despite these events, the patient and her estranged husband continue to speak to each other regularly.
The patient was seen in the preoperative education area before her surgery. She frequently generated a spontaneous, strong cough, producing moderate amounts of yellow & green sputum. She was instructed on the use of aerosolized medication therapy via metered dose inhaler (MDI) and coughing and deep breathing (C&DB) techniques. Her attention span, however, was poor, and she continually sang words of praise and recognition to every employee who passed her room. She also flooded the respiratory therapist with “aren’t you wonderful” phrases as the therapist tried to ask her to demonstrate the various techniques that she would be required to perform after her surgery.
After her surgery, while in the postanesthesia area, she continually used foul language and threatened to have everyone fired. Her physician ordered a sedative and then transferred her to the postoperative unit. Over the next 2 hours, the patient’s general respiratory status declined.
Concerned, the primary nurse paged the physician. Busy in another part of the hospital, the physician requested a respiratory care consultation.
Physical Examination (Time: 1330)
The respiratory care practitioner noted that the patient was awake and in obvious respiratory distress. Her vital signs were as follows: blood pressure 185/90, heart rate 130 bpm, respiratory rate 35/min, and temperature normal. She demonstrated a frequent spontaneous, weak cough. She often expectorated a moderate amount of yellow sputum during a coughing episode.
She appeared cyanotic and quickly stated, “Damn, my gut really hurts, . . . and I can’t seem to get any air.”
Over the left lower lung, diminished breath sounds were noted. Bronchial breath sounds and dull percussion notes were noted over the right lower lung. The nurse indicated that the patient’s incentive spirometry (IS) volume was only about 40% of her preoperative value (when she could get the patient to attempt to use the device). Her oxygen saturation measured by pulse oximetry (Sp
O
2
) on a 2 L/min oxygen nasal cannula was 77%. Arterial blood gas values (ABGs) obtained by the respiratory care practitioner were as follows: pH 7.57, Pa
CO
2
23 mm Hg, HCO
3
–
21 mmol/L, and Pa O
2
43 mm Hg. No recent chest X-ray was available. As the therapist documented the data, the patient’s physician entered the room and stated, “I’ll do anything to
Mosby items and derived items © 2006 by Mosby, Inc.
Case Study 2 keep this patient off the ventilator. Keep me informed.” The physician then prescribed some medication for the patient’s pain and quickly left the room.
1.
What disease process should the team suspect that he has?
2.
What evidence supports it?
3.
What is the interpretation of the current blood gas? Why?
4.
What are some immediate actions that he RCP could take?
5.
What are some treatment recommendations that the RCP could make?
1 Day After Surgery
Despite the patient’s need for aggressive respiratory care, she was generally uncooperative or unwilling to tolerate various treatment modalities. She had not been transferred to the intensive care unit (ICU). Her skin was blue, cool, and damp. Her eyes were closed, and she was unresponsive to questions. She still demonstrated a weak cough every few minutes.
Although sputum retention was suspected, none was actually seen; the patient was believed to be swallowing any sputum produced. Her vital signs were as follows: blood pressure 188/100, heart rate 135 bpm, respiratory rate 36/min, and rectal temperature 38.1° C (100.6° F).
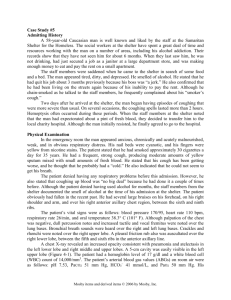
Chest assessment revealed dull percussion notes, bronchial breath sounds, and crackles over the right middle and both lower lobes. A portable chest X-ray revealed that she had mild atelectasis in the right middle and both lower lobes. Air bronchograms also were noted in this area (Figure 10-1). Her Sp
O
2
was 72%. Her ABGs were as follows: pH 7.55, Pa
CO
2
29 mm Hg,
HCO
3
–
22 mmol/L, and Pa
O
2
46 mm Hg.
Figure 10-1 Chest X-ray of a 43-year-old woman
Mosby items and derived items © 2006 by Mosby, Inc.
Case Study 3
1.
Is the pt in respiratory distress?
2.
What evidence supports it?
3.
What is the interpretation of the current blood gas? Why?
4.
What are the abnormal findings on the chest x-ray?
5.
What are some immediate actions that he RCP could take?
6.
What are treatment recommendations that the RCP could make in addition to a respiratory consultation?
7 Hours Later
A therapeutic bronchoscopy was performed in the ICU. The patient was not intubated.
The respiratory care practitioner on the pulmonary consult team found the patient in obvious respiratory distress. Her skin was cyanotic, cool, and damp. She stated, “I think I’m dying.” No cough was observed at this time. No right-sided chest excursion could be seen, and her trachea was deviated to the right.
Her vital signs were as follows: blood pressure 192/90, heart rate 142 bpm, respiratory rate 20/min, and oral temperature 37.3° C (99.1° F). Bronchial breath sounds, crackles, and dull percussion notes were found over the right middle and lower lobes. Dull percussion notes and no breath sounds were noted over the left lower lobe. Her Sp
O
2
was 62%. Her ABGs were as follows: pH 7.26, Pa
CO 2
53 mm Hg, HCO
3
–
22 mmol/L, and Pa
O 2
37 mm Hg.
1.
Is the pt still in respiratory distress?
2.
What evidence supports it?
3.
What is the interpretation of the current blood gas? Why?
4.
What are some immediate actions that he RCP could take?
5.
What are treatment recommendations that the RCP could make in addition to current therapies?
Mosby items and derived items © 2006 by Mosby, Inc.
Case Study 4
Review
1.
Did this patient’s history suggest that she might develop atelectasis? b. c.
Did this patient initially or subsequently demonstrate any evidence of the clinical manifestations of atelectasis? If so, what were they?
Did this patient initially demonstrate any evidence of the pathophysiologic
4. b. c. d. e. d. alterations commonly associated with atelectasis?
Which specific clinical manifestations did this patient demonstrate that helped you decide on the severity of her condition?
Application a. Sputum induction (was/was not) indicated because ______________________ .
Oxygen therapy (was/was not) indicated because ______________________ .
Bronchial hygiene therapy (was/was not) indicated because ________________ .
Hyperinflation therapy (was/was not) indicated because __________________ .
Aerosolized medication therapy
______________________ .
(was/was not) indicated because _____________ f. g.
Mechanical ventilation (was/was not) indicated in this case because
______________________ .
Pulmonary rehabilitation (was/was not) indicated because _________________ .
Mosby items and derived items © 2006 by Mosby, Inc.