Business Case
advertisement

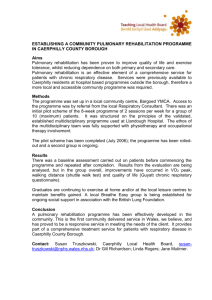
[ADD ORGANISATIONS NAME] Business Case for a [RESPIRATORY SPECIALIST] Physiotherapist [ADD AUTHORS NAMES, JOB TITLES AND DATE] Contents 1 Introduction 2 Background information 3 Local issues 4 Proposal 5 Cost analysis 6 Benefits and outcomes 1 1 Introduction This business case highlights the necessity for a [CLINICAL SPECIALIST] in respiratory physiotherapy. The requirement is driven by the need for [XX N.H.S Trust (ADD OTHERS IF ADDITIONAL ORGANISATIONS INVOLVED)] to respond to the current and future changing needs of its population. The proposal covers the following areas: Background information Local issues Proposal Cost analysis Benefits and outcomes The cost for implementing a [CLINICAL SPECIALIST IN RESPIRATORY PHYSIOTHERAPY ROLE] is [£XX (SEE COSTS SECTION AND ADD TOTAL)]. These costs will be recovered by the resultant impact on reducing admissions, reducing Length of Stay (LOS) and readmission rates and a reduction in the social care costs. Strong evidence is offered to support this business case both in terms of local demographic need alongside clinical evidence supporting the impact of such a post and the proposed service provision. 2. Background Information Respiratory disease is the third most common cause of chronic ill health in the UK causing patients to experience escalating disability and limitations to their quality of life. The resultant impact is that respiratory patients are heavy users of healthcare and social care resources ([1]. Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and mortality placing large demands on both hospitals and General Practice (GP) services. The period prevalence of COPD in the United Kingdom is around 11%, with approximately 900,000 diagnosed COPD patients in England and Wales [2]. COPD is the only disease in the Department of Health (DH) top five killer diseases, which is still increasing (163% in the last twenty years). It has been estimated that inpatient costs for COPD exacerbations account for 70% of the total health costs for the COPD patient population. COPD accounted for 107,352 admissions to hospital in England and Wales and a total of 1051,567 inpatient days in 1999-2000, costing the N.H.S over £818 million in 1999. An estimated 100,000 hospital admissions were recorded for COPD in England in the year 2000, equating to around 1m bed days [3] 2 Whilst there is currently no curative treatment for COPD, it is possible for the patients in our local population to improve symptom management, function and quality of life if given the appropriate therapy support. The introduction of a specialist physiotherapist for this population group would enable patients to better manage their condition themselves. This would in turn reduce acute admission rates, reduce LOS and for those who do require admission and significantly reduce re-admission rates. In the United States there are well-established pulmonary rehabilitation programmes available, based on a wealth of evidence based research [4]. Over the last few years more centres in Britain have developed pulmonary rehabilitation services and British standards for pulmonary rehabilitation are now available [5]. In Wales Llandough Hospital and to a limited extent Singleton Hospital and Wrexham Maelor Hospital provide this service with beneficial effects. The Llandough pulmonary rehabilitation programme currently saves Cardiff and Vale N.H.S trust £150 per patient who completes the course [1] and data suggests that pulmonary rehabilitation is effective at reducing hospital days associated with exacerbation [6,7] 2. Local Issues NB ALL BELOW DATA CAN BE ACCESSED FROM LOCAL PUBLIC HEALTH SPECIALISTS . [XX NHS TRUST] serves a population of [XX] of whom XX% will require treatment for respiratory disease. This represents a total of XX people who will require support from XX N.H.S trust. Our multidisciplinary team serves the population of XX of whom a potential XX will require treatment for respiratory disorders. To serve the population there are XX medical beds and XX [ADD ANY OTHER BEDS, SERVICES LOCALLY.] Despite the above services there is no formalised provision for specialist respiratory physiotherapy support. [IF HAVE LIMITED SPECIALIST RESPIRATORY SUPPORT STATE WHAT HAVE AND THE LIMITATIONS.] The acute [COPD] admissions for XX N.H.S. Trust have increased from XX in 2002-2003 to XX in 2004-2005. [ADD DATA FROM ANY OTHER RELEVANT ORGANISATION LOCALLY]. Patients in XX N.H.S Trust have higher LOS than others in areas matched for similar socio-demographics, and longer than the national average of XX. [DATA AVAILABLE FROM DH WEBSITE]. The average length of stay for the Trust is XX days. We are therefore not meeting national performance targets in terms of respiratory admissions and length of stay, but are also falling further behind comparable trusts. NB CHECK ABOVE STATEMENTS IS THE CASE IF NOT 3 OFFER COMPARATIVE DATA. The input of a specialist physiotherapy could significantly help to reverse this trend. respiratory There is no (STATE IF LIMITED RATHER THAN NONE) specialist physiotherapy provision for the education and treatment of patients with chronic respiratory disease. If these patients were properly served, hospital admissions would be avoided and LOS and readmission rates reduced. Patients would be facilitated to maintain an independent lifestyle at home dramatically increasing the quality of life. Resource gains can thus be realised through the prevention of hospital admissions and readmissions, and a reduction in the cost of providing long-term care and support in the community. The current staffing levels prevent us from providing the necessary clinical interventions, rehabilitation and education for patients. In addition there is no specialist respiratory physiotherapist providing continuing professional development to more junior members of staff enabling them to deliver more effective clinical interventions. A physiotherapist who has specialist knowledge of respiratory conditions would fulfil this commitment to the population we serve. This service would also compliment the current respiratory services we offer [ADD SPECIFIC SERVICES AS APPROPIATE] at [XX N.H.S. Trust.] [ADD OTHER ORGANISATIONS AS APPROPIATE] 3. Proposal This business case makes the case for funding a specialist physiotherapist to undertake pulmonary rehabilitation and [XX] [ADD OTHER SERVICES / INTERVENTIONS AS APPROPATE] so that we may address the needs of the population we serve. The proposal is set out as follows: Overview: [CHANGE AS REQUIRED TO REFLECT LOCAL NEEDS – BELOW IS OFFERED AS WORKING EXAMPLE] The post holder would be based at [XX] organisation and would manage physiotherapy intervention for patients requiring non-invasive ventilation in the Acute Medical Admissions Unit (AMAU), thereby preventing progression to more invasive ventilation and other complications which increase LOS and reduce outcomes. The post holder would work cross sites and across organisational boundaries and will produce and deliver a training package to educate 4 colleagues to support the provision of pulmonary rehabilitation across the trust. The post holder would link with community services to enable smooth discharge planning and would provide expert support for clinicians working in the community with patients who have respiratory disorders. The post holder would lead the physiotherapy intervention as part of a pulmonary rehabilitation programme across [XX NHS Trust], thereby enabling the population of [XX] to maintain their health, well being and lifestyle choices for longer. The post holder will develop the physiotherapy educational framework for the respiratory team and will expand our links with the University of [XX ADD ANY LOCAL LINKS WHICH WILL ENHANCE OUTCOMES] The post holder will evaluate their input and provide key outcome data including the impact on admission rates, LOS and readmission rates. Quality of life and functional level outcomes will also be collected. Range and Scope [CHANGE AS REQUIRED TO REFLECT LOCAL NEEDS – BELOW IS OFFERED AS WORKING EXAMPLE] Clinical Lead pulmonary rehabilitation services across the trust / community Provide support and education to service users and their carers Support the NIV therapy to [XX] Hospital Develop the respiratory service into the community setting Co-ordinate and participate in health promotion across the local population Develop physiotherapy led clinics based at the cardio-respiratory centre at [XX ]Hospital Set standards and revise policies for the physiotherapy respiratory service based on best practice and clinical outcomes Work as part of a respiratory multidisciplinary team and participate in networks Participate in research Produce clear outcome data Educational /developmental role Lead the education of physiotherapy colleagues to ensure respiratory competencies are maintained for on call purposes and pulmonary rehabilitation 5 Coordinate and lead in the education of junior and rotational staff from physiotherapy and other professionals in respiratory issues Coordinate the education of physiotherapy students within a respiratory module. Ensure best practice and new research findings are consistently and appropriately implemented and maintained. Ensure staff understand and use outcome measurements as part of daily practice 5 Costs The proposal includes all related costs including salary, on-costs, equipment, administration support and travel and study leave expenses. A break down of the costs is: Employment of a physiotherapist who is a [CLINICAL SPECIALIST] in respiratory disorder –[£XX NB AGENDA FOR CHANGE SALARY] On costs – [£XX] Equipment [£XX – LIST ITEMS AND INDIVIDUAL COSTS] Venue costs for running Pulmonary Rehabilitation [£XX – ONLY ADD IF NECESSARY BUT CONSDIER FUTURE EXPANSION MAY ADD COSTS] Administration costs [£XX – ONLY ADD IF REQUIRED AND CANNOT BE COVERED BY CURRENT ESTABLISHEMENT – WILL NEED TO DO DISCHARGE REPORTS AND COMMUNICATION WITH GPS AND COMMUNITY STAFF IN TIMELY AND EFFECTIVE MANNER] Travel expenses approx [£XX – QUANTIFY] Study leave expenses [£XX] Total Cost [£XX] per annum (NB ADD INFLATION LIFT FOR FOLLOWING YEARS / CONSIDER ONGOING FUNDING REQUIREMENTS) 6 Benefits and Outcomes A physiotherapy respiratory specialist post is fundamental to the delivery of high quality, efficient and effective care for the local population with respiratory disease. The initial costs of implementing this post will be recovered by the resultant reduction in acute admissions and a reduction in LOS and readmission rates. In addition, the functional and quality of patients lives will be optimised. In summary the key benefits and outcomes are: Dramatic improvement in specialised acute care for respiratory patients 6 Reduction in acute admissions reducing the costs for the health economy and enhancing the patient experience Reduction in the length of stay in hospital for patients who are admitted thus preventing bed blockages, clinical and social complications and reducing the costs for the health economy and enhancing the patient experience Enablement of patients to maintain a healthier lifestyles and greater independence, thus reducing the reliance on social care services. This will offer additional costs saving across the health economy Ensuring the education of patients and staff with continual service and professional development, thus preventing the risk of inappropriate care and the consequences both for patients and the costs to the health economy Reduction in health inequalities and improved health standards across the community and the Trust Develop of multidisciplinary team working in the approach to respiratory care offering seamless high quality care to patients. This will ensure a robust approach to the whole patient pathway ensuring patient are clearly maintained and monitored through out their whole illness Improve recruitment and retention of permanent staff thus lowering the cost of locum services to the trust. The Locum costs for 2003-2004 have been an average of [£XX] and for 2004-2005 an average of £XX] [ADD ANY OTHER LOCUM / RECUITMENT AND RETENTION ISSUES LOCALLY AS APPROPIATE]. Reference List 1. Griffiths T L, Phillips C J, Davies S, Burr M L, Campbell I A. Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme. Thorax 2001; 56: 779-784. 2. National Collaborating Centre for Chronic Conditions. Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax 2004; 59: 1-232. 3. National Respiratory Training Centre. National Respiratory Training Centre Impact of Respiratory Conditions: a guide for Primary Care Organisations. 2002. Warwick, NRTC. 7 4. Lacasse Y, Maltais F, Goldstein R S. Pulmonary rehabilitation: an integral part of the long-term management of COPD. Swiss.Med.Wkly. 2004; 134: 601-605. 5. Morgan M D, Calverley P M, Clark C, Davidson A C, Garrod R, Goldman J, Griffiths T L, Roberts E, Sawicka E, Wallace L, White R. British Thoracic Society Statement on Pulmonary Rehabilitation. Thorax 2001; 56: 827-834. 6. Foglio K, Bianchi L, Bruletti G, Battista L, Pagani M, Ambrosino N. Long-term effectiveness of pulmonary rehabilitation in patients with chronic airway obstruction. European Respiratory Journal 1999; 13: 125-132. 7. Man W D, Polkey M I, Donaldson N, Gray B J, Moxham J. Community pulmonary rehabilitation after hospitalisation for acute exacerbations of chronic obstructive pulmonary disease: randomised controlled study. BMJ 2004; 329: 1209. 8