ESWT IN PAIN THERAPY
advertisement

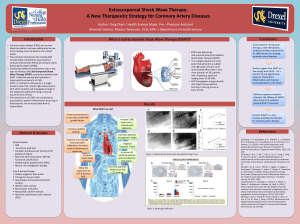
ESWT IN PAIN THERAPY Background Since the early 1980s, extracorporeal sound wave therapy (ESWT) has been used in the treatment of nephrolithiasis and cholelithiasis with successful outcome in well over 3 million patients (1). In the field of orthopaedics ESWT was first employed in the therapy of delayed bone fracture healing and pseudoathroses in 1991 by Valchanou and Michailov (2). Since the beginning of the 1990's the use of this technique has expanded to include treatment of enthesopathies - specifically lateral epicondylitis, plantar fasciitis, and rotator cuff tendinitis. Numerous scientific studies have been carried out in Europe, especially in Germany where now over 100 clinics use ESWT routinely. There are several major manufacturers of ESWT equipment - Dornier, Storz, Siemens, Ossatron. Three of these manufacturers have obtained HPB (Health Protection Branch) approval for the use of their equipment in Canada. Bayshore has no preferred status with any manufacturer, thus we can select the best equipment available on the market at a given time. Bayshore's plan is to establish a network of approx. 18 ESWT clinics from coast to coast. ESWT treatment is not covered by Provincial health care plans. However, several private insurers cover the ESWT fee and others are assessing the possibility of ESWT as an insured service. ESWT is applied using a system which integrates an electromagnetic sound-wave generator in a mobile fluoroscopy unit. The sound waves are generated by passing a strong electric current through a flat coil. This induces a magnetic field, which itself induces another magnetic field in a magnetic membrane overlying the flat coil. Just as similar poles repel each other, so do the generated magnetic fields of the membrane and the coil. By means of an acoustic lens the focus of the sound wave source is just at the centre of the C-arm. The focal area in which 50% of the maximum energy is reached. It has a length of 50 mm in the direction of the sound-wave axis and a radius of 3.5 mm in the direction perpendicular to the sound-wave axis. Once the painful area is situated in the centre of the C-arm, the sound wave unit is docked on to the foot, lateral epicondyle, or shoulder by means of a water-filled cylinder. An ultrasound gel is used as a contact medium between the cylinder and the skin. The energy density of the sound-wave generator can be varied from 0.06 mJ/mm2 to 0.6 mJ/mm2. This is represented by a power setting scale ranging from 1 to 9, in which energy density has a non-linear increase (3). For pain therapy only power levels of 0.04 to 0.23 mJ/mm2 are used (1). Position and sound wave focus are continuously monitored during the treatment by a centre cross hair, using the ultrasound screen. Therapy impulses are applied with an adjustable frequency of up to 4 Hz (4). Depending on the size of the area being treated, between 1,000 and 3,000 impulses are applied to the therapy zone (1). The sound wave generator comprises a closed system which as such does not endanger the patients when used properly. ESWT is performed under ambulatory conditions and one session lasts 25-45 minutes; the patient is usually able to return to work on the following day (1). On average 3-5 sessions are required per patient and are performed at 3-4 day intervals. A cooling ointment dressing is applied to the treated area after each session. Contraindication to ESWT is the presence of any of the following: a polyneuropathy, blood coagulation disorders, inflammatory systemic disorders, cancer, pregnancy (1). One of the main advantages of ESWT is the lack of side effects from the treatment (1) (3). Recent studies showed that there are dose-dependent changes in tendon and paratenon tissue after ESWT in animal models, however with energy flux densities of 0.28 mJ/mm2 or lower these changes are minor and quickly reversible (5). Damage to tendons is only observed after the application of high-energy sound waves, i.e. greater than 0.28 mJ/mm2 (5). In pain therapy only 0.8-0.23 mJ/mm2 are used. In a study on ESWT in treating calcific rotator cuff tendinitis, Loew et al had 7% patients develop superficial hematomas of the soft tissue and 25% of patients had skin petechia. All patients in this study had a MRI a few days after treatment and no changes of the bone, cartilage or tendon structure were detected (6). Rompe et al, reports no complications in more than 500 patients treated with ESWT for lateral epicondylitis (7). The mode of action of ESWT seems to be a symbiosis of three different mechanisms, which together induce long term analgesic effects: 1. The sound waves destroy part or all the cell membrane, making it impossible for the nociceptor to build up any generator potential, thus preventing the occurrence of a pain signal. 2. The sound wave causes the nociceptor to transmit a high impulse frequency. Any forwarding of these impulses is prevented as described under "gate control theory" 3. The sound wave induces neovasvularization. The sound wave stimulates increased blood supply to the affected area resulting in reduced inflammation and pain. 4. The sound wave alters the chemical environment surrounding the cell by forming free radicals which produce analgesic substances (1) For any musculoskeletal condition, the treatment procedure of choice should be the least invasive, least expensive and most time efficient. The last two points do not apply to ESWT and thus ESWT is currently not used as a first line treatment but reserved for refractory cases of lateral epicondylitis, plantar fasciitis, and rotator cuff tendinitis. Lateral epicondylitis (LE) - commonly referred to as "tennis elbow" - was described more than a century ago, but its pathophysiology and treatment are not yet mastered. The incidence of this condition varies from approximately 1 to 3% in the general population (12). Lateral epicondylitis involves the wrist extensors at or near their lateral epicondylar origin and the extensor carpi radialis brevis is most commonly affected. Less commonly involved muscles are the extensor carpi radialis longus, the extensor digitorum communis, and rarely the extensor carpi ulnaris. The initial events in LE are microscopic as well as macroscopic tears in the extensor origin at the lateral epicondyle; this tearing is followed by formation of granulation tissue and fibrosis (12). Patients usually present with pain in the region of the lateral elbow which can radiate down the extensor surface of the forearm as far as the wrist, exacerbated by repetitive activity. An estimated one third of cases interfere with activities of daily living (12). Many treatments are recommended for LE, such as relative rest, ice, physiotherapy, oral NSAIDS, forearm supports, injections of corticosteroids, prophylactic counseling, laser radiation, and acupuncture. Less than 10% of patients fail to improve with these conservative measures and require surgical intervention (12). Recently, low dose ESWT has been found to be effective in treating this condition in isolated cases (7). Rompe et al recently published two studies which looked at patients with symptoms for more than 12 months. The test group received 3000 impulses of 0.08 mJ/mm2 while the control group received only 30 impulses of the same energy. There were significant differences between the two groups in follow-up with respect to subjective outcomes, objective grip strength, and overall outcome, with the test group having much better outcomes (7) (8). This suggests that ESWT can be an effective treatment for refractory LE and is not just a placebo effect. Plantar fasciitis (PF) is the most common diagnosis for pain in the inferior aspect of the heel. The etiology usually involves inflammation and degeneration of the plantar fascia origin from the medical tubercle of the calcaneal tuberosity. The plantar fascia is an aponeurosis that divides distally into several slips and inserts into the proximal phalanges. The PF helps to maintain the medial longitudinal arch. The pain of plantar fasciitis is classically worse upon arising in the morning and gradually gets better with the first few steps. PF may or may not be associated with a calcaneal heel spur. The majority of patients will respond to conservative measures such as relative rest, massage locally, ice, oral NSAIDS, corticosteroids injections, physiotherapy, heel cups or pads, custom-made orthodics, laser treatment, night splints, etc. Occasionally surgical intervention is required for refractory cases. PF release is one of the more popular methods of surgical management (13). Lowenergy ESWT has been introduced as an alternative to surgery for chronic, refractory cases of PF. Patients with symptoms for over 12 months were treated with 1000 impulses of 0.08mJ/mm2 in three separate sessions; a control group received 10 impulses of the same energy. In follow-up there were statistically significant differences between the test group and controls with respect to rest and night pain and length of pain-free walking (3). After low-energy ESWT the average time to significant improvement was 3-6 weeks, compared with 3 months for surgery in one series (3). No side effects were noted from ESWT; the treatment was considered unpleasant, but not as unpleasant as a local infiltration, by the patients. One of the most common causes of pain in the shoulder is rotator cuff tendinitis, with or without calcification. This is commonly the result of repetitive work or activity where the supraspinatous tendon impinges on the caudal surface of the coracoacromial arch. The supraspinatous tendon is the most superior in the RC and inserts onto the greater tubercle; it keeps the humeral head in the shallow glenoid fossa during shoulder movement. Impingement results in inflammation. Patients have shoulder pain which is worsened by overhead activity and by lying on the affected side. In some cases calcification develops within the tendons as a result of angiofibroblastic change from multiple tendon tension overload. Conservative therapy is aimed at reversing inflammation in the rotator cuff. This includes relative rest, ice, oral NSAIDS, physiotherapy, corticosteroid injections, etc. Surgical intervention in the form of either arthroscopic or open subacromial decompression is considered if an adequate trial of conservative therapy fails. ESWT has been studied as a treatment in calcific RCT (6) (10). In one series, disintegration and vanishing of calcification on radiographs was demonstrated in 60% of patients after 12 weeks (6). Subjectively, 70% of patients showed clear improvement of their symptoms (6). In another study, 40 patients with persistent calcifying tendinitis were treated with a single session of 1500 pulses of 0.28 mJ/mm2. With follow-up at 6 and 24 weeks, 62.5% of the patients had partial or complete disintegration of the deposit, and statistical analysis showed significant improvement both in subjective and objective criteria (10). Literature References 1. Haist, J, Steeger von Keitz, D. Shock Wave therapy of Radial and Ulnar Epicondylar Disorders. Presentation from the Convention of German Orthopaedic Surgeons, Wiesbaden, Germany, October 12-15, 1994. 2. Rompe, J.D.: Efficient Use of Extracorporeal Shock Waves in Tendinopathies. electromedica 65 (1979) no.l, p. 20-25 3. Rompe, J.D.,Kullmer, K., Riehle, H.M., Herbsthofer, B., Eckardt, A., Burger, R., Nafe, B., 4. *United Medical Systems: Analgesic Therapy of Chronic Pain in Orthopaedics by ESWT. August 1998. 5. Rompe, J.D., Kirkpatrick, C.J., Kullmer, K., Schwitalle, M., Krischek, 0.: Dose-related effects of shock waves on rabbit tendo Achillis. J of Bone and Joint Surgery, May 1998, no.3, vol. 80-B,p. 546-52 6. Loew, M., Jurgowski, W.Ueberle, F.: The Effects of Extracorporeal ly Generated HighEnergy Shock Waves on the Clinical, Roentgenological and Histological Progress ofTendinosis Calcarea of the Shoulder-a Prospective Study. Orthopaedische Universitaetsklinik, Heidelberg, Germany. 7. Rompe, J.D., Hopf, C., Nafe, B., Burger, R.: Analgesic Effect of Exrracorporeal ShockWave Therapy On Chronic Tennis Elbow. J of Bone and Joint Surgery, March 1996, no.2, vol.78-B, p.223-7. 8. Rompe, J.D., Hopf, C., Kullmer, K., Heine, J., Burger, R., Nafe, B.: Low-energy extracorporeal shock-wave therapy for persistent tennis elbow. International Orthopaedics (SICOT),1996,20_23-27. 9. Rompe, J.D., Hopf, C., Nafe, B., Burger, R.: Low-energy extracorporeal shock wave therapy for painful heel a prospective controlled single-blind study. Arch Ortop Trauma Surg, 1996,115:75-79. 10. Rompe, J.D., Rumler, F., Hopf, C., Nafe, B., Heine, J.: Extracorporeal Shock Wave 11. Geoffroy, P., Yaffe, M., Rohan, I.: Diagnosing and treating lateral epicondylitis. Canadian Family Physician, January 1994, vol.40, p. 73-78 12. Chard, M.D., Hazleman, B.L.: Tennis Elbow - A Reappraisal. Brit J of Rheumatology, editorial, vol.28,no.3, p. 186-188 13. Schepsis, A. A., Leach, R.E., Gorzycs, J.: Plantar Fasciitis - Etiology, Treatment Surgical Results, and Review of the Literature. Clinical Orthopaedics and Related Research, May 1991, no.266, p. 185-196