Exploration of the therapeutic potential of extracorporeal shock wave
advertisement

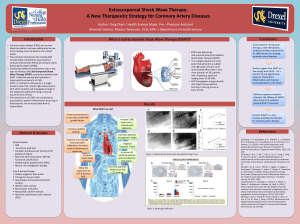
EXPLORATION OF THE THERAPEUTIC POTENTIAL OF EXTRACORPOREAL SHOCK WAVE TO PREVENT/AMELIORATE INFLAMMATORY BOWEL DISEASE STRATEGY The innovation of this proposal is to explore the potential of extracorporeal shock wave to prevent/ameliorate the intestinal inflammatory responses associated with inflammatory bowel disease in the dextran sodium sulfate (DSS) colitis mouse model. Extracorporeal shock wave therapy (ESWT) is a low energy, unfocused acoustic pulse consisting of a fast (<10nsec) peak pressure wave of up to 100 megapascal (MPa) with an energy flux density of 0.01-0.11 mJ/mm2 and a 10µsec duration that propagates into soft tissue. ESWT at cellular interfaces of different acoustic impedances produces tensile forces, which produces high temperature, rapidly imploding microscopic cavitation bubbles (not sure for unfocused low energy shockwaves). Consequently, data has shown that at appropriate energy flux densities specific beneficial molecular pathways are triggered. Indeed, since 1980 extracorporeal shock wave therapy (ESWT) has been employed for the treatment of a variety of diseases, including orthopedic diseases (pseudoarthosis, tendinitis calcarea of the shoulder, epicondylitis, and plantar fasciitis), traumatic wound healing, burn injury, vessel injury/atherosclerosis and ischemia. Interestingly, although the exact biochemical mechanisms remain unclear, ESWT has been shown to induce tissue regeneration, neoangiogenesis, and a general anti-inflammatory modulation of the immune system. Our collaborative group has previously shown that ESWT treatment of burn wounds 1 hour post-wounding potently attenuated chemokine expression, suppressed pro-inflammatory cytokine production, decreased extracellular matrix proteolytic activity at the wound margin, and significantly blunted neutrophil and macrophage infiltration into the wound. The findings strongly indicate that ESWT may be a potential therapeutic modality which ameliorates inflammation and accelerates the normal physiological repairs process of wound healing. Additionally, we have recently demonstrated that abdominal ESWT preconditioning can limit the systemic inflammatory response syndrome (SIRS) and intestinal ileus caused by traumatic peripheral tissue injury. Our preliminary data suggest that ESWT can ameliorate weight loss and prevent death associated with the DSSinduced colitis in a mouse model of IBD. In a pilot study, sham mice lost on average a significantly higher percentage of their body weight (14.4±3.55%) compared to q.a.d. ESWT treated mice (5.7±3.19%) in response to oral DSS 3% on day 7. Given this encouraging preliminary data, the aim of this proposal is to fully delineate the potential of ESWT to prevention weight loss, ameliorate the detrimental histological changes within the intestinal mucosa, decrease the colitis cellular inflammatory response, maintain colonic muscle function and prevent death in response to DSS-induced colitis. AIM I. DEMONSTRATE THE POTENTIAL OF ESWT TO PREVENT THE SEQUELAE ASSOCIATED WITH DSS-COLITIS. Rationale. Our data demonstrates the ESWT can ameliorate DSS-induced colitis, therapeutically prevent postoperative ileus, and diminish the systemic consequences of traumatic peripheral tissue injury. Hypothesis. We propose that ESWT induces an anti-inflammatory/tolerant protective state in the gut which ameliorates the detrimental consequences of DSS-induced colitis in the mouse. Approach. “Acute” DSS-induced colitis will be studied by exposing individual groups of mice to a low (2.5%) or moderate (3.5%) dose of DSS in the drinking water for a continuous period of 14 days. ESWT will be delivered as a single exposure treatment at the commencement of DSS exposure or delivered every other day (q.a.d.). Similarly, “chronic” DSS-induced colitis will be studied by intermittently exposing individual groups of mice to a low (2.5%) or moderate (3.5%) dose of DSS in the drinking water on a regimen of 7 days on/7 days off for three dosing cycles (35 days). ESWT will be delivered at the commencement of each DSS cycle. A control group and sham groups of mice anesthetized to mimic the treatment regimens will be used for comparison. Therapeutic un-focused electro-hydraulic acoustic shock waves will be delivered to the shaved ultrasound gel coated abdomen of an anesthetized mouse as 600 pulses consisting of a fast (10nsec) peak pressure wave of 100 megapascal (MPa) with an energy flux density of 0.03 mJ/mm2 and a 10 µsec duration at a frequency of 3 to 4 Hz (note: energy flux density may be altered to optimize a therapeutic effect I would recommend energy flux densities of 0.08 to 0.1 mJ/mm2)). End-point Analyses. Each mouse in the individual groups will be weighed daily and plotted for changes in body weight. From the anesthetized animals at the specified times of sacrifice for each group of mice, the colon will be removed and placed in an oxygenated Krebs physiological solution. Proximal and distal segments of the colon will be fixed in paraformaldehyde (2.5%), sectioned and histologically stained for changes in the mucosal architecture and leukocytic infiltrates (neutrophils and monocytes/macrophages). Colonic circular muscle strips from the mid-colon will be prepared, and muscle contractility and electrical field stimulated neurogenic contractions will be quantified. AIM II. ELUCIDATE THE MOLECULAR MECHANISMS OF ESWT. Rationale. If the above data confirms our preliminary findings, we will investigate two hypotheses which could mechanistically explain the therapeutic effect of ESWT for inflammatory bowel disease. Based on previous observations we will determine if ESWT induces a reactive oxygen-dependent molecular cascade which results in the suppression of inflammation via the induction of Suppressors of Cytokine Signaling (SOCS)-1 and SOCS-3. [ROIs → Egr-1/NF-κB → SOCS-1&3 → suppression of colitis] Alternatively, we will investigate whether an ESWT-induced cellular permeabilization results in the “leakage” of nucleic acids which triggers a local TLR3/TRIF signaling response causing an “immune tolerization” of the intestinal structures to the chemically-induced DSS inflammation (hypothesis of J. Holfeld). A similar pathway is known to be activated during LPS/TLR4 tolerization, which we have shown to be dramatically beneficial for preventing experimental postoperative ileus. These two hypotheses are based on the current state-of-the-art knowledge in this field. Appropriate molecular experiments will be designed to address each hypothesis. References Bauer AJ (2010). Two immune arms to stop one gut. Nat Med 16, 1378-1379. Choi KM, Kashyap PC, Dutta N, Stoltz GJ, Ordog T, Shea DT, Bauer AJ, Linden DR, Szurszewski JH, Gibbons SJ, & Farrugia G (2010). CD206-positive M2 macrophages that express heme oxygenase-1 protect against diabetic gastroparesis in mice. Gastroenterology 138, 2399-409, 2409. Davis TA, Stojadinovic A, Anam K, Amare M, Naik S, Peoples GE, Tadaki D, & Elster EA (2009). Extracorporeal shock wave therapy suppresses the early proinflammatory immune response to a severe cutaneous burn injury. International Wound Journal 6, 11-21. Engel DR, Koscielny A, Wehner S, Maurer J, Schiwon M, Franken L, Schumak B, Limmer A, Sparwasser T, Hirner A, Knolle PA, Kalff JC, & Kurts C (2010). T helper type 1 memory cells disseminate postoperative ileus over the entire intestinal tract. Nature Medicine 16, 1407-1413. Kalff JC, Buchholz BM, Eskandari MK, Hierholzer C, Schraut WH, Simmons RL, & Bauer AJ (1999a). Biphasic response to gut manipulation and temporal correlation of cellular infiltrates and muscle dysfunction in rat. Surgery 126, 498-509. Kalff JC, Hierholzer C, Tsukada K, Billiar TR, & Bauer AJ (1999b). Hemorrhagic shock results in intestinal muscularis intercellular adhesion molecule (ICAM-1) expression, neutrophil infiltration, and smooth muscle dysfunction. Arch Orthop Trauma Surg 119, 89-93. Kobayashi K, Hernandez LD, Galan JE, Janeway CA, Jr., Medzhitov R, & Flavell RA (2002). IRAK-M is a negative regulator of Toll-like receptor signaling. Cell 110, 191-202. Kuo YR, Wang CT, Wang FS, Chiang YC, & Wang CJ (2009a). Extracorporeal shock-wave therapy enhanced wound healing via increasing topical blood perfusion and tissue regeneration in a rat model of STZ-induced diabetes. Wound Repair Regen 17, 522-530. Kuo YR, Wang CT, Wang FS, Yang KD, Chiang YC, & Wang CJ (2009b). Extracorporeal shock wave treatment modulates skin fibroblast recruitment and leukocyte infiltration for enhancing extended skin-flap survival. Wound Repair & Regeneration 17, 80-87. Mittermayr R, Hartinger J, Antonic V, Meinl A, Pfeifer S, Stojadinovic A, Schaden W, & Redl H (2011). Extracorporeal shock wave therapy (ESWT) minimizes ischemic tissue necrosis irrespective of application time and promotes tissue revascularization by stimulating angiogenesis. Annals of Surgery 253, 1024-1032. Moore BA, Albers KM, Davis BM, Grandis JR, Togel S, & Bauer AJ (2007). Altered inflammatory gene expression underlies increased susceptibility to murine postoperative ileus with advancing age. Am J Physiol Gastrointest Liver Physiol 292, G1650-G1659. Moore BA, Otterbein LE, Turler A, Choi AM, & Bauer AJ (2003). Inhaled carbon monoxide suppresses the development of postoperative ileus in the murine small intestine. Gastroenterology 124, 377-391. Moore BA, Overhaus M, Whitcomb J, Ifedigbo E, Choi AM, Otterbein LE, & Bauer AJ (2005). Brief inhalation of lowdose carbon monoxide protects rodents and swine from postoperative ileus. Crit Care Med 33, 1317-1326. Ricchetti GA, Williams LM, & Foxwell BM (2004). Heme oxygenase 1 expression induced by IL-10 requires STAT-3 and phosphoinositol-3 kinase and is inhibited by lipopolysaccharide. J Leukoc Biol 76, 719-726. Schmidt J, Stoffels B, Moore BA, Chanthaphavong RS, Mazie AR, Buchholz BM, & Bauer AJ (2008). Proinflammatory role of leukocyte-derived Egr-1 in the development of murine postoperative ileus. Gastroenterology 135, 926-36, 936. Schwarz NT, Engel B, Eskandari MK, Kalff JC, Grandis JR, & Bauer AJ (2002). Lipopolysaccharide preconditioning and cross-tolerance: the induction of protective mechanisms for rat intestinal ileus. Gastroenterology 123, 586-598. Stoffels B, Schmidt J, Nakao A, Nazir A, Chanthaphavong RS, & Bauer AJ (2009). Role of interleukin 10 in murine postoperative ileus. Gut 58, 648-660. Wang FS, Wang CJ, Sheen-Chen SM, Kuo YR, Chen RF, & Yang KD (2002). Superoxide mediates shock wave induction of ERK-dependent osteogenic transcription factor (CBFA1) and mesenchymal cell differentiation toward osteoprogenitors. Journal of Biological Chemistry 277, 10931-10937. Wehner S, Behrendt FF, Lyutenski BN, Lysson M, Bauer AJ, Hirner A, & Kalff JC (2007). Inhibition of macrophage function prevents intestinal inflammation and postoperative ileus in rodents. Gut 56, 176-185.