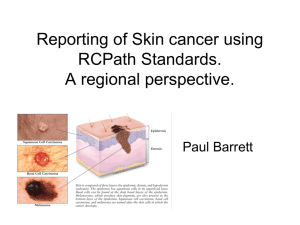
The Pre-Operative Prevention and Post
advertisement

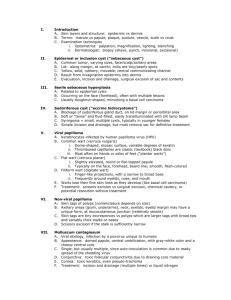
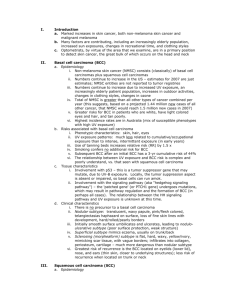
Outline I. Introduction A. Skin layers and structure: epidermis vs. dermis B. Terms: macule, papule/nodule/tumor, plaque, pustule, vesicle/bulla, scale, crust C. Examination techniques 1. Optometrist: palpation, magnification, daylight exam, blanching 2. Dermatologist: biopsy (shave vs. punch vs. incisional vs. excisional) D. Skin cancers: non-melanoma skin cancer (basal cell carcinoma + squamous cell carcinoma), malignant melanoma, sebaceous gland carcinoma II. Basal cell carcinoma (BCC) A. Background 1. Most common skin cancer 2. Grows slowly, never resolves, areas of chronic sun exposure 3. 90% appear on the face and neck, with primary location being the nose 4. Heavy cumulative UV-B, red/blond hair, tans poorly, family history 5. UV causes p53 tumor suppressor gene mutation, suppresses Langerhans cells and cytotoxic T cells 6. Growth is by direct extension with “stromal dependence” and rare metastasis B. Characteristics 1. There is no precursor lesion to a basal cell carcinoma 2. Nodular: translucent, waxy papule, pink/flesh colored, telangiectasias haphazard on surface, loss of fine skin lines, hard/rolled/pearly borders 3. Initially smooth surface umbilicates and ulcerates, leading to nodulo-ulcerative type (poor surface protection, inherent structural instability) 4. Superficial type resembles eczema, usually on trunk/back, rare on face 5. Sclerosing (morpheaform) is flat, hard, waxy, yellow/ivory, resembling scar tissue, with vague borders; infiltrates into collagen, periosteum, cartilage III. Squamous cell carcinoma (SCC) A. Background 1. Second most common after BCC; non-ocular is 5:1 for BCC:SCC 2. Occurs on sun-damaged skin and scar tissue, burns, areas of chemical exposure, chronically infected sinuses, and stasis ulcers 3. Frequently seen on scalp, tops of ears, and backs of hands 4. Fair-skinned patients most vulnerable (see demography for BCC patients) 5. Precursors to SCC can be an actinic keratosis or cutaneous horn 6. Etiology: same as BCC (suppresses p53 gene and Langerhans cells) 7. Quite uncommon on eyelids vs. BCC (SCC is 5-10% of eyelid cancers) B. Characteristics 1. Downgrowth of abnormal keratinocytes into dermis 2. Begins as small, firm, erythematous nodule or a flat red/scaly patch 3. Early SCC in epidermis only is Bowen’s disease (SCC-in-situ) 4. Enlarges, variable surface scale (heavy when arising in an actinic keratosis) 5. SCC grows faster than BCC, ulcerates/bleeds/crusts sooner than BCC 6. SCC has no standard appearance: readily confused with actinic keratosis, keratoacanthoma, seborrheic keratosis, scabbed BCC, sebaceous gland ca. 7. Risk of metastasis varies widely: low (< 6%) if associated with actinic keratosis, up to > 40% if arising from scar tissue or genital areas IV. Conditions related to or confused with squamous cell carcinoma A. Actinic keratosis is a common, pre-malignant, sun-induced lesion 1. Seen often in older patients, indicative of cumulative UV-B exposure 2. Pink macule with sandpaper surface, “seen before felt” located on the face, neck, scalp, and arms 3. Thin keratin scale which darkens and thickens 4. Malignant transformation indicated by induration, inflammation, red base 5. Treatment: sunscreens, Retin-A, liquid nitrogen, 2% or 5% fluorouracil B. Cutaneous horn is a secondary lesion occurring with the primary lesions of actinic keratosis, viral warts, seborrheic keratosis, and/or SCC 1. Located on face, ears, hands, etc. which are typical for primary lesions 2. Conical projection of lamellar layers of keratin C. Keratoacanthoma is a benign lesion with an alarming growth pattern 1. Domed papule, keratin-filled central crater grows exuberantly in 2-3 months 2. Stabilizes for up to 1 year, then discharges keratin core, leaving shallow scar 3. More common in elderly fair-skinned patients D. Seborrheic keratosis is very common, slowly growing, without malignant potential 1. Of epidermal origin, appearing as a “floating plaque” stuck on the epidermis 2. Tan, brown, even black, with variable elevation, granular/crumbly surface V. Treatments for non-melanoma skin cancer A. Surgical excision: removes entire growth plus surrounding “normal” skin; margins are evaluated microscopically to ensure that all malignant cells are removed B. Electrodesiccation and curettage: tumor is removed with a curette, then desiccated, then removed again; the surgeon feels the difference between soft/friable tumor and firm dermis, but no margins are left for microscopic evaluation C. Cryosurgery: liquid nitrogen applied with a cryogun; best limited to those expert with the technique and for well-defined in situ tumors (e.g., Bowen’s disease) D. Radiation: useful for tumors needing preservation of surrounding tissue; good cosmesis, but time-consuming, requiring multiple treatments and slow healing E. Mohs micrographic surgery: tumor is microscopically delineated until totally removed, with very low recurrence rates; indicated for tumors likely to recur or in locations in which recurrence is more likely (periobital area, ears, scalp, etc.) F. Carbon dioxide laser: pulsed technique seals blood vessels as it cuts; best for superficial BCC and SCC in situ; thick or nodular lesions should not be lasered G. Topical fluorouracil (5-FU): traditionally used for Bowen’s disease with 5-FU in propylene glycol; experimental use of 5-FU in BCC as an intralesional injection or topically with phosphatidyl choline as a transepidermal carrier (6-8 treatments) H. Systemic retinoids: neither isotretinoin or beta carotene prevented further develop-ment of BCC in individuals previously treated for NMSC; no trials have been done to demonstrate prevention of NMSC in individuals with sun-damaged skin only I. Interferon alfa: both interferon alfa-2b and alfa-2a have been used intralesionally for BCC, and alfa-2b has also been effective for SCC; must evaluate cost-benefit ratio. J. Photodynamic therapy: porphyrins act as photosensitizers to induce cell death by formation of free radicals; topical -ALA or I.V. Foscan have been tested for BCC (superficial and nodular) and SCC; large clinical trials are needed. VI. Pigmented lesions and color changes A. Guidelines for recognition of normal nevi 1. Size: less than 6 mm in diameter (pencil eraser size) Color: uniform within the lesion; varies from tan to black Shape: symmetric, with matching halves if “folded;” round or oval Borders: regular and usually distinct Nevi remain stable in size, shape, color; fade very slowly as they involute B. Dysplastic nevi (DN) 1. May be < 5 mm, but “classic” DNs are quite large (> 10 mm), with haphazard colors, 2 shades of brown, and asymmetric shape 2. Flat plus elevated components (“tan macular shoulder”) – fried egg 3. Variable risks of malignant melanoma C. Mnemonic for malignant changes in nevi 1. A = asymmetry (non-matching halves) 2. B = border irregularity (notching or regression) 3. C = color changes or irregularities (variable or multiple colors, mixes) 4. D = diameter (greater than 6 mm in size) 5. E = elevation (change from flat or only slightly elevated) 2. 3. 4. 5. VII. Malignant melanoma (MM) A. Background and epidemiology 1. Malignant neoplasm of epidermal melanocytes, with epidermal spread 2. Much lower incidence than BCC or SCC, but much higher mortality 3. Younger patients and increasing mortality 4. Australia (1 in 17 females, 1 in 14 males have MM within lifetime) 5. Risks: fair skin, fair hair, poorly tanning skin, family history of MM, blistering B. C. D. E. sunburns in teen years, equatorial residence, congenital nevi, thinning ozone layer 6. Proposed #1 cause: increased recreational exposure to UV (intermittent) 7. Most common locations: legs (females), back (males) 8. ~ 70% occur on normal skin (de novo), ~ 30% arise from nevi Superficial spreading melanoma (SSM) 1. Most common type in U.S.; typical age of onset is 40-50 years 2. Irregular border (notching), odd shape, mix of colors (red, white, blue) 3. Nodule formation is very dangerous; SSM is “safest” when remaining thin Nodular melanoma (NM) 1. About 15% of MM in U.S.; typical age of onset is 50-60 years 2. Dome-shaped; dark brown, black, gray, red-brown, amelanotic 3. Misdiagnosed as blood blister, dermal nevus, or polyp 4. Very dangerous due to vertical growth Lentigo maligna melanoma (LMM) 1. Precursor = Hutchinson’s freckle 2. Perhaps the most common malignant melanoma on the face 3. Irregular borders, bizarre shape, varying mixes of brown 4. Nodule development on Hutchinson’s freckle malignancy with LMM 5. Generally the safest MM, with an obvious precursor for many years Treatment of MM 1. Excision; margins = 1 cm if tumor < 1 mm thick, 2-3 cm if > 1 mm thick 2. Rigorous follow-up depending on MM thickness VIII. Sebaceous gland carcinoma (SGC) A. Meibomian glands, glands of Zeis, eyebrows, caruncle, follicle-associated B. Characteristics: uncommon compared to BCC (7% or less of lid malignancies), older patients more affected, upper lid > lower lid involvement, risky (metastasis) C. D. E. F. IX. Appears as firm, painless nodule; yellow color; pagetoid spread into conjunctiva May mimic chalazion, chronic blepharitis/meibomitis, SLK, ocular pemphigoid Biopsy any lesion that is suspicious or unresponsive to therapy Treatment consists of surgical excision, Mohs surgery, and lymph node evaluation Guidelines for suspecting malignancy Atypical: odd behavior, out of synch for age, wrong for patient demographics History of other malignancy (NMSC, family history, immunosuppression) Older patient, heavy UV regardless of age, complexion, hair color, occupation Lesions characteristics 1. Unresponsive to therapy, or previously stable and now changing 2. Change in lesion (disobeys ABCDE rule, or has odd growth pattern) 3. Eroded and/or bleeding surface, inflamed, odd size, irregular tissue 4. Localized telangiectasias (BCC, SGC) vs. diffuse (2o chronic sun exposure) 5. Lid changes: madarosis, chronic palpebral conjunctival hyperemia E. “The Usual Suspects” = scabbing, bleeding, infection A. B. C. D. X. Prevention strategies A. Sunscreens or avoidance may reduce aging changes (deep wrinkles, lentigenes, persistent erythema), actinic keratoses, NMSC, and malignant melanoma Text: Habif TP. Clinical dermatology, third ed. 1996; St. Louis: Mosby.