Audit of skin cancer reporting - Northern England Strategic Clinical
advertisement

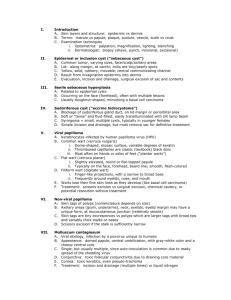
Reporting of Skin cancer using RCPath Standards. A regional perspective. Paul Barrett Aim • Determine if RCPath standards have been adopted – Part of network clinical guidelines (Jul13) – RCPath Oct12 (revised May14) • Pathology can be critical in determining cases to be discussed at MDT – Excisional intent – High risk – Incompletely excised • Planned high quality cancer care to just over 3 million people in the North of England • 8 Foundation and 1 NHSTrusts • 14 Primary Care Trusts (PCTs) • 5 localities Method • 25 reports requested from 2014 – Each cancer type – Each centre reporting in North East • Core items in RCPath guidelines assessed • One centre failed to submit by deadline • Not all cases suitable • Not all sites had 25 cases Melanoma • Fairly established dataset • No major changes Results - Melanoma • • Lab Cases 1 25 2 8 3 19 Non-proforma 4 4 – 4 central (6%) – 22 local (71%) 5 26 6 11 7 8 101 cases Local MDT – 31 • Proforma – 75 • Results - Melanoma • All cases – Macroscopic description skin ellipse – Macroscopic description lesion – Excision margins Results - Melanoma Critical results • Breslow 1 • Clark’s 6 • Ulceration 7 (1/0) (5/1) (7/0) • 12 cases do not include vital data • All destined for review Results - Melanoma • LVI • PNI • Microsat 5 11 52 (5/0) (11/0) (22/30) • Subtype • Growth phase • Stage 13 9 21 (12/1) (9/0) (18/3) Results - Melanoma • Mitotic rate • Regression • TiL 2 17 14 • All data items provided (2/0) (15/2) (14/0) 47 (46%) SCC • Significant change around risk status • Complexity with pT2 – Any two of • • • • Poor differentiation Into subcutaneous tissue >2mm Into reticular dermis Results - SCC • • Lab Cases 1 25 2 9 3 25 Non-proforma 4 2 – 11 central (17%) – 52 local (82%) 5 24 6 20 7 21 126 cases Local MDT – 52 (41%) • Proforma – 63 (all central) • Results - SCC • All cases – Macroscopic description skin ellipse – Macroscopic description lesion – Excision margins Results - SCC Critical results • Grade 8 • Thickness 10 • Level 32 (8/0) (10/0) (30/2) Results - SCC • LVI • PNI 7 22 (7/0) (22/0) • Subtype • Risk • Stage 47 86 65 (47/0) (54/32) (41/24) Results - SCC • Correct assessment of risk – Recorded in 40 • 3 incorrect • 2 insufficient data in report to assess • All data items provided • 32 cases (2/30) 25% BCC • Established data set • Is it really cancer? • Multiple specimens common Results - BCC • • Lab Cases 1 25 2 21 3 25 Non-proforma 4 25 – 8 central – 86 local 5 23 6 22 7 18 159 cases Local MDT – 86 (54%) • Proforma – 65 (all central) • (17%) (100%) Results - BCC • All cases – Macroscopic description skin ellipse – Macroscopic description lesion Results - BCC Key results • Growth pattern • Level 1 57 (1/0) (56/1) • Margins 2 (1/1) Results - BCC • LVI • PNI 28 15 (27/1) (14/1) • Risk • Stage 85 92 (85/0) (68/24) • All data items provided 26% • 41 cases • Combination risk and/or stage absent Recommendations • Data could be derived • Melanoma review centrally • Confirms value in reporting by proforma – College KPI • Ensure proforma contains all core items • Re-audit or audit locally Clinical imunosuppression Site: Specimen type: Size: Size of lesion: Marker & ink: Description: Curette / Shave / Punch / Incisional Length Width o’clock LLP SH BB Classic Acantholytic Grade: Well Thickness: mm Adj Bowen’s dis: No SqCC Subtype: BCC Subtype: Superficial Infiltrative Atypical Sq D: No Level of invasion: radiation, burn or chronic inflammation Excisional to a depth of mm high risk if >20mm inked margin- Tips: Transverse: KA-like Verrucous Other: Spindle cell Moderate Poor >4mm Stage may increase if >2mm Yes Adj Bowen’s dis: No Micronodular Yes BCC T stage: SCC only Risk status: MDT discussion: Comments: Subtype: into papillary dermis into reticular dermis* confined to epidermis Yes Superficial Nodular Infiltrative Micronodular Atypical Sq D: No into subcutaneous fat *possible stage increase for SqCCa No Yes No Yes involved clear <1mm clear 1-5mm Yes confined to epidermis into papillary dermis at unspecified margin/ clear <1mm o’clock clear 1-5mm fills papillary dermis into reticular dermis* pT2 pT3+ pT2 if 2 of poor diffn, PNI, lip/ear site, into reticular dermis, >2mm thick into subcutaneous fat Low No LVI: No Yes PNI: No Yes Level of invasion: clear 5mm+ involved clear 5mm+ pT1 <=20mm deep: Stage may increase if >2mm Nodular fills papillary dermis LVI: PNI: Margins peripheral: mm >4mm Thickness: High Yes (excisional, high risk and incomplete) Margins peripheral: involved deep: T stage: SCC only clear <1mm *possible stage increase for SqCCa clear 1-5mm o’clock clear 5mm+ at unspecified margin/ involved clear 5mm+ clear <1mm clear 1-5mm pT1 <=20mm pT2 pT3+ pT2 if 2 of poor diffn, PNI, lip/ear site, into reticular dermis, >2mm thick Questions?