EPITHELIAL
PRECANCEROUS SKIN
LESIONS
BY
DR. MAHESH MATHUR
MD.DVD,DCP
DIFENATION
PRECANCEROUS SKIN LESIONS ARE ONE THAT
HAS STRONG POTENTIAL TO TRANSFORM INTO
MALIGNANCY- CHARECTERISED CLINICALLY- BY HAVING POTENTIAL TO BECOMES
INVASIVE CARCINOMAS
HISTOPATHOLOGIACLLY - SHOWS CELLULAR
ATYPIA CONFINED TO EPIDERMIS
DIFFERENTIATION
&
ANAPLASIA
PLEOMORPHISM
ABNORMAL NUCLEAR MORPHOLOGY
MITOSIS
LOSS OF POLARITY
LOSS OF UNIFORMITY OF THE
INDIVIDUAL CELLS AS WELL AS LOSS OF
ACHITECTURAL ORIENTATION
PRECANCEROUS SKIN LESION
ACTINIC KERATOSIS
ARSENICAL KERATOSIS
CHRONIC RADIATION KERATOSIS
BOWEN’S DISEASE
ERYTHROPLASIA OF QUEYRAT
ERYTHROPLAKIA
LEUKOPLAKIA
ACTINIC KERATOSIS
AGE >60 - 80% CHNCES OF DEVELOPMENT
M>F
PHENOTYPE OF FAIR SKIN WHICH BURN &
FRECKLES EAISLY AND RERELY TAN
BLUE OR LIGHT COLOURED EYES & BLOND
HAIR
IMMUNOSUPPRESSION
GENETIC SYNDROMES XERODERMA PIGMENTOSUM & ALBINISM
PATHOGENESIS
SUNLIGHT EXPOSURE
UV-INDUCED MUTATION IN
TUMOR-SUPPRESSOR GENE p53
PATHOGENISIS
CLINICAL PICTURE
IN ELDERLY PATIENT
80% OF LESIONS FOUND ON CHRONICALLY
SUN EXPOSED SITES –
HEAD,NECK,FORARMS & DORSA OF HAND
ERYTHEMATOUS, FLAT,SCALY,YELLOW
COLOURED PAPULES
HYPERTROPHIC - CUTANEOUS HORN
ACTINIC CHEILITES
ACTINIC KERATOSIS
ACINIC KERATOSIS
ACTINIC CHILITIS
ARSENICAL KERATOSIS
CHRONIC ARSENISM – TRIVALENT ARSENIC
EXPOSURE
PREEXISTING LIVER DISEASE
CLINICALLY – PIN POINT PAPULES AT PALMS &
SOLES
ELEVATED ERYTHEMATOUS PLAQUES ON NON
PHOTO DAMAGE AREA OF SKIN, MULTIPLE
LESIONS AT TRUNK
UNDERLYING SYSTEMIC MALIGNANCY
BECOME INVASIVE TO CAUSE SCC.
ARENICAL KERATOSIS
CHRONIC RADIATION KERATOSIS
OCCURS AFTER CHRONIC EXPOSURE TO
RADIATION
X’RAY THEREPY
MEDICAL PERSONNELS,
DENTISTS
NUCLEAR ACCIDENTS
PAPULES,PLAQUES AT PALMS, FINGERS &
MUCOSA
SCC & BCC MAY DEVELOPES WITH OTHER
MALIGNANCY
RADIATION KERATOSIS
BOWEN’S DISEASE
1912
SQUAMOUS CELL CARCINOMA IN SITU
AFFECTS BOTH SKIN & MUCOUS MEMBRANES HAVING POTENTIAL TO PROGRESS INTO INVASIVE
CARCINOMA
AGE >60 RARELY BEFORE 30 YEARS OF AGE
CAN OCCUR AT ANY BODY PARTS – SUN OR NON SUN
EXPOSED AREAS OF BODY
SUN EXPOSURE,
ARSENIC EXPOSURE
IONIZING RADIATION,
IMMUNOSUPPRESSION
INFECTION WITH HPV-16 SPECIALLY ANOGENITAL BOWEN’S
DISEASE
CLINICAL PICTURE
DISCRETE
SLOWLY ENLARGING
PINK TO ERYTHEMATOUS
THIN PLAQUE WITH WELL
DEMARCATED,IRREGULAR BORDERS
OVER LINING SCALES OR CRUST
HYPERKERATOTIC VERRUCOUS LESIONS
5% OF BD PROGRESS TO INVASIVE SCC
BOWNE’S DISEASE
PATHOLOGY
FULL THICKNES CELLULAR ATYPIA
BASEMENT MEMBRANE REMAINS INTACT
HYPERKERATOSIS
PARAKERATOSIS
ACNTHOSIS
COMPLETE DISORGANIZATION OF
EPIDERMAL ARCHITECTURE
WIND BLOWN APPEARANCE
LOSS OF MATURATION & POLARITY
HISTOPATHOLOGY
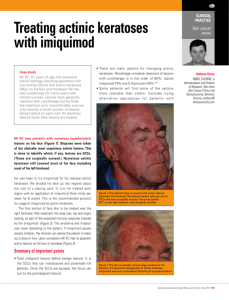
TREATMENT
SURGICAL EXCISION - 95%
CRYOSURGERY
- 90 %
CURETTAGE
- 65%
5 FU TOPICAL CHEMOTHERAPY – 66%
IMIQUIMOD 5% CREAM - 93%
LASER
- 89 T0 100%
PHOTO DYNAMIC THERAPY
ERYTHROPLASIA OF QUEYRAT
EQ- IS CARCINOMA IN SITU AFFECTING
THE MUCOSAL SURFACES OF PENIS IN
UNCIRCUMCISED MALES
AGE 20 TO 80 YEARS
UNCIRCUMCISED
POOR HYGIENE
SMEGMA
HSV INFECTION
HPV-16 & 18 INFECTION
CLINICAL PICTURE
GLISTENING
RED
VELVETY PLAQU ON GLANS PENIS,PREPUCE OR
URETHRA
USUALLY SOLITARY PLAQUE
LOCALISED PAIN OR PRURITUS
DIFFICULTY IN RETRACTING FORE
BLEEDING OR CRUSTING MAY BE THERE AT THE
LESION
ENLARGE SLOWLY & PERSIST FOR SEVERAL
YEARS
33% OF CASES PROGRESS TO INVASIVE SCC
LEUKOPLAKIA
IT IS FIXED PREDIMINANTLY WHITE LESION OF MUCOSA
ORAL & ANOGENITAL MUCOSAL SURFACES
ALCOHOL & TOBACCO USE
AGE >50 TO 70 YEARS
5 TO 25% RISK OF BECOMING INVASIVE
CLINICALLY ASYMPTOMATIC
ASYMMETRIC
WHITE PLAQUE
AT FLOOR OF MOUTH
LATERAL & VENETRAL TOUNGE
SOFE PLATE
DIAGNOSIS BY BIOPSY
SURGICAL EXCISION OF THE LESION
MULTIPLE PIGMENTED NEVUS
>50 IN NUMBER
_> 2 mm SIZE
64 TIMES
INCREASE RISK
GIANT MELANOCYTIC NEVUS
DYSPLASTIC NEVUS
MELANOMA IN SITU
MACULAR FRACKELS LIKE LESIONS WITH
IRREGULAR SHAPE WITH DIFFERENT SHADES
OF COLOUR
ELDERLY PATIENT
OCCURS ON SUN EXPOSED AREA OF SKIN
ENLARGING RADIALLY FEW TO MANY IN
NUMBERS
LIFE TIME RISK OF DEVELOPMENT OF
MELANOMA IS 4.7 %
ATYPICAL MELANOCYTIC NEVUS
ATYPICAL MELANOCYTIC NEVUS
HISTOPATHOLOGY
THANK YOU…