High Cumulative Risk of Intussusceptions in patients with Peutz-Jeghers Syndrome.
M.G.F. van Lier1, A. Wagner2, A.M. Westerman3, J.H.P. Wilson3, F.W.M. de Rooij3, E.J.
Kuipers1,3, M.E. van Leerdam1
Department of Gastroenterology and Hepatology1, department of Clinical Genetics2 and
department of Internal Medicine3, Erasmus MC, University Medical Center, Rotterdam, the
Netherlands.
Peutz-Jeghers Syndrome (PJS) is an inherited disorder characterized by
gastrointestinal hamartomas and mucocutaneous pigmentation. A germline mutation in the
STK11 gene can be found in 70% of clinically affected patients. The hamartomas are mainly
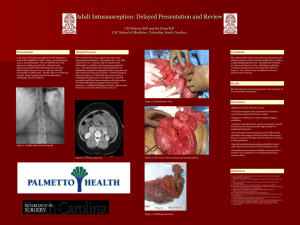
located in the small bowel and may cause intussusceptions. Since balloon-enteroscopy (BE)
enables endoscopic removal of small bowel polyps, we assessed genotype-phenotype
correlations and the risk and onset of intussusception.
Patients diagnosed with PJS based on clinical diagnostic criteria or proven STK11
mutation were included in this prospective cohort study (1995 - Nov 2008). Clinical data
including sex, date of birth and death, diagnosis of PJS, STK11 mutation status, family
history and diagnosis of intussusception were obtained by interview and chart-review.
Genotype-phenotype correlations were evaluated. The cumulative risk of intussusception was
calculated by Kaplan-Meier analyses.
Forty-four PJS patients (57% males) were included out of 18 PJS families; 32 patients
still alive had a median age of 44 years (range 10-74 yrs) and 12 patients had deceased at a
median age of 45 years (range 11-73 yrs). A germline STK11 mutation had been detected in
32 patients (73%). Thirty-four patients (77%) had a history of one or more episodes of
intussusception (range 1-6) due to small bowel polyps (one malignant degenerated polyp).
The median age at which the first intussusception had occurred was 13,5 years (range 3-50
yrs). Surgery was required in 33 patients (75%), whereas in 1 case the invagination resolved
spontaneously. There was no significant difference in intussusception incidence according to
sex (p=0,15) or mutation-status (p=0,70). Kaplan Meier analyses showed that intussusception
had occurred in 50% of the cohort at a median age of 16 years (95% CI 11-21), increasing to
75% (95% CI 62-88) at the age of 35 yrs. The 10-year probability of intussusception was 25%
(95% CI 12-38).
Conclusion: PJS patients carry a high cumulative risk of intussusception (50% at 16
yrs) caused by small bowel hamartomas. The incidence of intussusception is not influenced
by STK11 mutation status. These findings support the approach of enteroscopic surveillance
with timely removal of small bowel hamartomas. The effect of this approach on the incidence
of intussusception (as well as malignant degeneration) remains to be established and weighted
against the burden and complication risk of the intervention.