Intussusception
advertisement

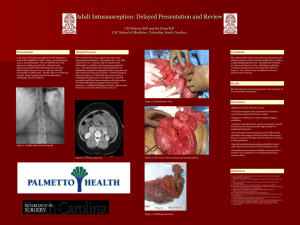
RADIOLOGY IN THE ED Intussusception Edematous Ileocecal Valve Mimicking Incomplete Reduction Mary T. Kitazono, MD and Avrum N. Pollock, MD, FRCPC From the Department of Radiology, Children’s Hospital of Philadelphia, Philadelphia, PA. Disclosure: The authors declare no conflict of interest. Reprints: Avrum N. Pollock, MD, FRCPC, Department of Radiology, Children’s Hospital of Philadelphia, 34th and Civic Center Blvd, Philadelphia, PA 19104 (e-mail: POLLOCKA@email.chop.edu). Copyright * 2012 by Lippincott Williams & Wilkins ISSN: 0749-5161 PRESENTATION A 3-year-old boy presents with intermittent colic, emesis, and bloody diarrhea for 1 day. RADIOLOGY FINDINGS An abdominal ultrasound reveals a characteristic target sign in the transverse plane (concentric rings formed by multiple layers of bowel wall) in the right lower quadrant compatible with an ileocolic intussusception (Fig. 1). The patient subsequently underwent single-contrast water-soluble reduction enema, which revealed an intraluminal filling defect (M) in the proximal ascending colon (Fig. 2A) compatible with an intussusceptum, which was successfully reduced by the contrast column to the level of the cecum, allowing reflux of contrast into the small bowel. However, a masslike filling defect (asterisk) persisted along the medial aspect of the cecum FIGURE 1. Ultrasound demonstrating the classic bowel-within-bowel appearance of intussusception on ultrasound, composed of multiple concentric rings of bowel wall, often referred to as a target sign. (Fig. 2B). A targeted ultrasound performed after the reduction enema confirmed successful reduction of the intussusception, with fluid seen traversing a thickened, edematous ileocecal valve (arrows; Fig. 3), which accounts for persistence of a FIGURE 2. A, Water-soluble contrast enema demonstrating an intraluminal filling defect in the ascending colon compatible with the intussusceptum. B, Postreduction fluoroscopy revealing a persistent masslike filling defect on the medial aspect of the cecum, in the expected region of the ileocecal valve. This may represent an edematous ileocecal valve, a persistent intussusceptum in the setting of an incomplete reduction, or a pathologic lead point. 300 www.pec-online.com Pediatric Emergency Care & Volume 28, Number 3, March 2012 Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. Pediatric Emergency Care & Volume 28, Number 3, March 2012 FIGURE 3. Postreduction ultrasound showing an edematous ileocecal valve, accounting for the filling defect seen on fluoroscopy, and confirming complete reduction of the intussusception. masslike filling defect in the cecum on the postreduction fluoroscopic image. DISCUSSION Ileocolic intussusception is a common pediatric abdominal emergency, for which reduction enema (air- or water-soluble contrast) is the initial treatment of choice. Approximately 80% to 95% of intussusceptions can be successfully reduced nonoperatively, with higher success rates seen in patients presenting with a shorter duration of symptoms (G24 hours), in the typical age group ranging from 6 months to 3 years, and in the absence of a visible lead point or trapped intraperitoneal fluid seen within the intussusception.1Y3 Patients with signs concerning for perforation, peritonitis, or shock, or who fail multiple reduction attempts, require operative reduction.2,3 Although ultrasound-guided enema reduction is a reliable and safe alternative in the hands of an experienced operator, fluoroscopically guided reduction enemas are more commonly performed in North America, primarily owing to the training and experience of the radiologist. One of the disadvantages of fluoroscopic guidance over sonographic guidance is the occasional dilemma when there are equivocal signs regarding the success of the procedure. Criteria for a successful hydrostatic reduction enema include disappearance of the intussusceptum as well as reflux of contrast from the cecum into the ileum. Fulfillment of both criteria is necessary, as rarely contrast may be seen to reflux into the small bowel by flowing through or around a persistent ileoileocolic intussusception; this finding usually indicates the need * 2012 Lippincott Williams & Wilkins Intussusception for surgical intervention.4 An edematous ileocecal valve can occasionally mimic a persistent intussusceptum or a pathological lead point on the postreduction fluoroscopic images, appearing as a residual filling defect along the medial wall of the cecum. A postprocedure targeted ultrasound can help confirm complete reduction of the intussusceptum and exclude a pathologic lead point when a masslike filling defect remains in the cecum. The sonographic appearance of an edematous ileocecal valve has been likened to an aperistaltic ‘‘donut,’’ consisting of an echogenic center surrounded by a broad, hypoechoic rim.5 The postreduction ‘‘donut’’ is smaller in diameter compared with the prereduction target lesion and lacks the typical concentric rings and invaginated mesentery. In addition to grayscale images, visualization of a continuous movement of air bubbles floating from the cecum into the ileum is another helpful sign that confirms patency.6 Color Doppler sonography may also be useful in demonstrating the continuous flow of fluid through the ileocecal valve, similar to the jet phenomenon utilized to depict the unobstructed flow of urine at the ureterovesicular junction.7 In summary, a persistent intraluminal filling defect seen in the cecum on fluoroscopy-attempted reduction of an ileocolic intussusception may pose a diagnostic dilemma in differentiating an edematous ileocecal valve from residual/recurrent intussusception or a pathologic lead point. This dilemma can be easily solved with postreduction sonography. REFERENCES 1. Daneman A, Navarro O. Intussusception. Part 2: An update on the evolution of management. Pediatr Radiol. 2004;34:97Y108. 2. Navarro OM, Daneman A, Chae A. Intussusception: the use of delayed repeated reduction attempts and the management of intussusceptions due to pathologic lead points in pediatric patients. AJR Am J Roentgenol. 2004;182:1169Y1176. 3. Soo Ko H, Schenk JP, Troger J, et al. Current radiological management of intussusception in children. Eur Radiol. 2007;17:2411Y2421. 4. Koplewitz BZ, Simanovsky N, Lebensart PD, et al. Air encircling the intussusceptum on air enema for intussusception reduction: an indication for surgery? Br J Radiol. 2011;84:719Y726. 5. Rohrschneider W, Troger J, Betsch B. The post-reduction donut sign. Pediatr Radiol. 1994;24(3):156Y160. 6. Woo SK, Kim JS, Suh SH, et al. Childhood intussusception: US-guided hydrostatic reduction. Pediatr Radiol. 1992;182:77Y80. 7. Crystal P, Barki Y. Using color Doppler sonography-guided reduction of intussusception to differentiate edematous ileocecal valve and residual intussusception. AJR Am J Roentgenol. 2004;182(5):1345. www.pec-online.com Copyright © 2012 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited. 301