Infection - Skin to Skin Contact
advertisement

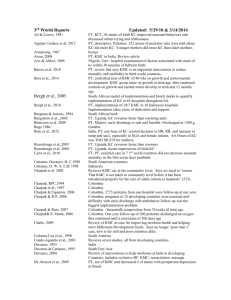
Infection Abouelfettoh et al., 2010 Anderson et al., 2003 AWHONN, 2008? Bauer, Sontheimer,et al., 1996 Cerezo & deLeon, 1992 Charpak et al., 1997 Charpak et al., 2001 Clarke, 2009 Conde-Agudelo et al., 2000b Conde-Agudelo et al., 2003 Conde-Agudelo et al.,2007 Crenshaw et al., 2004 Darmstadt et al., 2000 Mendes & Procianoy, 2008,09 Filho et al. 2008 Gangal, 2007 Gottesman,2009 Gupta et al., 2007 Hall & Kirsten, 2008 Hendricks-Munoz, 2002 Heyns et al., 2006 Jeanette et al. 2004 Kadam et al., 2005 Kambarami 2002 Updated: 5/19/10 PT, descriptive study of 5 days of KC effects on skin hydration (increased) and TEWL (increased) and # of infections during hospitalization and within one month of discharge (no infections after KC). Meta-Analysis showed KC associated with fewer nosocomial infections Positive benefits of KC include decreased incidence and severity of Infection., pg. 243. PT, VLBW, infection rate measured with maternal and paternal KC I think this is a descriptive study but I have to read it again No sig diff by blood cultures and no sig diff in other cultures PT, RCT, # & proportion of infectious episodes that had to be treated during hospitalization was same, proportion of nosocomial infections after eligibility and before discharge was less in KMC (3.8%) than controls (7.8%, p=0.026)(pg. 685). Number of total infectious episodes that had to be treated in hospital was lower in KC(7.6%, controls= 11%) but not sig. different. PT , RCT, less infections in KMC at 1 year of age- secondary to BF Rev of PT KC in developing countries and cites that KC has benefit of fewer infections. Just reporting that they will look at infection rate, no evidence to support reduced infection in 24/7 KMC infants Not meta-analysis results, but findings of the seven new studies they examined are that infections decrease in KC group PT, Cochrane Meta-analysis of 1362 24/7 KMC infants in 3 studies (same as reported before). KMC infants are at less risk of nosocomial infection and lower respiratory tract disease at 6 months. Review of reasons why KC at birth is good, and reduction in infections is one of the reasons for Lamaze’s support for normal birth position paper Review of how KC reduces infections and why it is important to use in community settings to prevent infections in newborns PT, VLBW RCT. KC was routine, standard care and infants who got KC + massage had less infection than KC alone group. PT, clin eval of 8 NICUs with KC stepdown vs 8 units without KC stepdown. No difference in infections between units. FT One step mentions “The baby’s risk of infection is reduced because safe germs (bacteria) from the mother start to colonize her skin and intestines, and prevent harmful germs from growing”(pg. 12).. Quotes Dr.Ludington as saying KC reduces infections and this is for consumers in MOTHERING magazine. PT, descriptive of 50 infants getting 4-6 hrs/day til discharge. No infections during KC. PT review of sloan, charpak 97 & 01 showing decreased infections PT, Clinical Report – “no evidence of increased risk of infection” PT, 4/6 babies in KMC unit got TB from untreated TB active mother. Review, says KC at birth helps prevent infection. Same as Crenshaw ref PT, RCT. # of sepsis in KMC =6, control =8. 6 KMC babies transferred back to regular care due to klebsiella pneumoniae. One KMC baby died from sepsis. Overall, no sig diff in sepsis incidence. PT, chart review of 42 twins/2 triplets in 24/7 KC unit. 6 had to go to NICU for sepsis, then returned to and discharged from KC unit Kambarami et al, 1998 Kirsten & Kirsten 2000 Lawn et al., 2010 Mallet et al., 2007 Mendes & Procianoy 2009 Mendes & Procianoy, 2008 Odent, 1989 Rao et al., 2008 Sakaki et al., 2009 Schanler 2001 Schanler et al., 2005 Sizun et al., 2004 Sloan et al., 1994 Sosa et al., 1976 Visser et al., 2008 WHO 1998 PT, RCT, 37 KC (24/7 KC) infants “were ill less frequently” than 37 controls. PT, RCT BF in KMC reduced incidence of nec (10% vs 2.8%) Meta analysis of KMC. It is particularly effective in reducing severe morbidity, particularly from infection. PT, Descriptive study of French NICU staff knowledge and barriers. Fear of nosocomial infection is a barrier to KC use. PT, RCT, VLBW. Less infection in KC + massage group than in KC alone group. PT, RCT, VLBW. Less infection in KC+massage (4 times a day from 48 hours oflife until discharge) than KC alone infants. FT, Clin Report- baby feeds at breast right after delivery in KC and Gets lots of IgA antibodies and zinc and enzymes in colostrums. PT, RCT, more controls than KMCers had nosocomial sepsis (p.19) PT, Descriptive prospective study of incidence of MRSA among 961 infants. KMC was a predictor of MRSA. PT, review article says that KC provides specific protection over infection due to enteromammary pathway PT, RCT, infants in mother’s own milk group (who also got significantly more episodes and significantly more duration of KC than preterm formula and donor milk groups) had fewer infection events (late onset sepsis, UTI, meningitis, NEC), but KC per se was not correlated to number of infection-related events. States that KC has shown fewer infections in developing countries but that these findings may not be relevant in high tech countries. Cites Charpak et al., 2001 as source of infection data. PT, RCT, decrease in severe infections such as pneumonia, septicemia in KMC infants over first 6 months of life In all 3 RCTs, FT infants who got 45 min of KC beginning after episiotomy repair had fewer episodes of infection (moniliasis, impetigo, and medicated illness). PT, descriptive of 23 preterm infants who came down with nosocomial RSV associated pneumonia one month after same strain appeared in general pediatric ward of same hospital in Gauteng, South Africa. Ft. states that when a mother and her baby are in KC the baby is exposed to the normal bacterial on the mother’s skin, which may protect the baby from becoming sick due to harmful germs. Related Literature Institute of Medicine, 2006 Report of Preterm Birth concludes that ‘stress’ and ‘infection’ contribute to the racial/ethnic differences in infant mortality rate.