N
Hospital infection Control
n
Nosocomial infections (hospital –acquired infection):
An infection acquired in [a] hospital by a patient who
was admitted for a reason other than that infection.
OR:
An infection occurring in a patient in a hospital or
other health care facility in whom the infection was
not present or incubating at the time of admission.
N
As a general timeline, infections occurring more than 48
hours after admission are usually considered nosocomial.
Frequency of infection:
Nosocomial infection occurs worldwide and affects both
developed and poor countries.
According to studies conducted by WHO, 8.7% of
hospitalized patients had nosocomial infection.
Factors influencing the development of nosocomial
infection:
1-The microbial agents and antibiotic-resistance ability:
-Patients are exposed to a variety of microorganisms
during a hospital stay:
A- Endogenous microbes: Part of a patient’s own flora.
B- Exogenous microbes:
-Patients, and Visitors.
-Medical staff (doctor, nurse, physiotherapist, technician).
-Instruments (Endoscopy, catheter, surgical instruments)
-Fluids, blood, or food.
-Dust, and Insect bite.
N
Hospital-dwelling microbes:
Bacteria:
Staphylococcus aureus (MRSA), coagulase-negative
Staphylococci, Enterococci (VRE), and Enterobacteriaceae
species.
Viruses:
Hepatitis B and C, Rotaviruses, and Enteroviruses.
Fungi:
Candida albicans.
N
Hospital-dwelling bacteria could develop antibiotics
resistance ability due to conjugation process.
Conjugation: Transfer of bacterial plasmid from one
bacterium to another by sex pili.
Plasmid: Extracircular supercoiled DNA that carry some
important gene such as the reporter genes (CAT gene).
N
2. Patient susceptibility:
Important patient factors influencing acquisition of infection
are:
1-Age : infancy and old age.
2-Immune status:
chronic diseases like malignant tumor, diabetes, renal failure
immunosuppressive therapy and AIDS.
3-Underlying disease : injuries to skin (burn, wound), ischemia.
4-Malnutrition.
5-Diagnostic and therapeutic interventions:
biopsies, catheterization, I.V. cannulation, endoscopic examination,
incubation/ventilation.
n
3. Environmental Factors:
-Different factors play a role in establishment of
Nosocomial infections:
1-Crowded conditions.
2-Frequent transfer of patients from one unit
to another.
3-Concentration of susceptible patients:
(newborn infants, burn patient, intensive care).
4-Microbial flora may contaminate objects, devices
that may come in susceptible site of the patient.
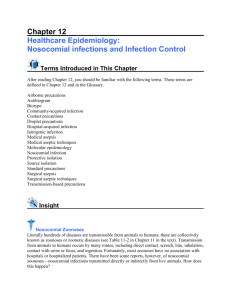
Sources of Hospital-acquired Infections:
Nimer
CONTAMINATED HOSPITAL ENVIRONMENT
Instruments, Fluids, Food,
Air, Medications
Invasive medical devices :
Iatrogenic
Patient Normal flora
Cutaneous, GIT,
Genitourinary,
Respiratory
Plasmid transfer
Medical Personnel: Colonized,
Infected, Transient, Carriers.
Urinary Catheter,
Intravenous catheter,
Endotracheal tubes,
Endoscopes
Common Nosocomial Infections:
1. Urinary tract infections (UTI):
This is the most common nosocomial infection it account for
40 % of hospital acquired infections; 80% of infections are
associated with the use of an indwelling catheter.
Organisms :
E.coli, multi-resistant Klebsiella, Pseudomonas aeruginosa,
Enterobacter and Candida albicans.
Source:
Endogenous flora or exogenous from other patients, health
care provider, instrument, etc.
N
Diagnosis:
positive urine culture (1 or 2 species) with at least 105
bacteria/ ml, with or without clinical symptoms.
Prevention:
1-Remove the indwelling urinary catheter as soon as
possible.
2-Use aseptic technique for inserting or manipulating the
catheter.
3-Maintain an unobstructed urinary flow.
4-Ensure that the patient is taking sufficient amount of
fluids
per day (3-4 L).
5-Give proper antibiotic therapy for proper course.
N
2.Nosocomial Pneumonia:
Nosocomial pneumonia is the second most common
nosocomial infection accounting for 15 % of all nosocomial
infections.
It is associated with mortality rates that range from
20-50 %.
It occurs in several patient groups, the most important are
patients on ventilator in intensive care units (ICU), where
the Incidence rate of pneumonia is 3% per day.
N
Organisms:
Staph aureus, Pseudomonas , Enterobacter, Klebsiella
pneumoniae, Candida albicans and Haemophilus
influenzae.
Source: endogenous from upper air way, and exogenous
from contaminated respiratory equipment, patients,
visitors, etc.
Diagnosis: isolation of microbe from clinical specimens,
and presence of signs and symptoms of infect.
n
Prevention:
1-Wear gloves; for contact with respiratory
secretions.
2-Wash hands after contact with respiratory secretions,
even if gloves have been worn.
3-Maintain open airway.
4-Isolate patient with potentially transferred
respiratory infections.
N
Other hospital-acquired infections:
1-Surgical site infections: Staphylococcus aureus,
Staphylococcus epidermidis (Intravenous catheter).
2-Nosocomial Bacteremia.
3-Skin and soft tissue infections:
Open sores (ulcers, burns and bedsores).
4-Gastroenteritis :
The most common nosocomial infection in the children,
where rotavirus is a chief pathogen.
N
5-Nosocomial Bloodborne diseases:
A-Hepatitis B virus:
-Transmission rate was 25%, reduced due to
application of vaccination, the practice of not
recapping needle, and Hepatitis B surface antigen
screening test.
B-Hepatitis C: Rate is 3%.
Anti-viral drugs at first 8 hrs reduce the infection by
60%.
C-HIV: Rate is 0.3%
Infection Control :
-Biological safety precautions.
-Hand hygiene.
-Clean & contaminated area.
-Management of blood & body fluid spillage.
-Immunization of health care workers.
-Post exposure management for health care
workers.
Biological safety precautions:
1-All clinical specimens should be considered as
potentially hazardous.
2-Wear Lab coat, gloves, shoes (Protective purpose).
3- Remove gloves when using the telephone or
photocopier.
4- Skin cuts on the hands, must be covered with a
waterproof dressing prior to start working.
n
5-Never perform any action which may bring your hands
into contact with your face, eyes or mouth, such as
eating, smoking or adjusting contact lenses.
6-Remove laboratory coat and
gloves and wash hands
before leaving your
working area.
Hand hygiene:
When Do We Need to Wash Our Hands?
-Before eating
-Before starting work
-Before and after any patient contact
-After contact with potentially contaminated materials like
blood, urine, CSF.
-Before wearing gloves.
-After removing gloves.
-Before and after performing any medical procedure
-Before leaving work.
When Do We Need to Wash Our Hands?
N
Types of Hand Hygiene (Decontamination):
1-Routine care (minimal):
-Hand washing with non antiseptic soap.
-Or quick hygienic hand disinfection by rubbing with alcoholic
solution.
2-Antiseptic hand cleaning (moderate) – aseptic care of
infected patients:
-Hygienic hand washing with antiseptic soap.
-Quick hand disinfection by rubbing with alcoholic solution.
3-Surgical scrub (surgical care):
Surgical hand and forearm washing with antiseptic soap and
sufficient time and duration of contact (3 – 5 minutes).
Clean & contaminated area:
Control of spreading of infection could be achieved by
classifying hospital environment into one of four zones:
Zone A: no patient contact. Normal cleaning .
(e.g. administration, library).
Zone B: Care of patients, who are not infected and not
highly susceptible. Wet disinfection with detergent.
Zone C: infected patients (isolation wards).
Clean with a detergent/disinfectant solution,
with separate cleaning equipment for each room.
N
Zone D: High–susceptible patient (protective isolation) or
protected areas such as:
Operating room, delivery rooms, intensive care
units, premature baby units, and haemodialysis
unit.
-Clean using a detergent/disinfectant solution and
separate cleaning equipment.
Blood and body fluid spillage, and contamination
management :
PURPOSE: To protect healthcare workers, patients and
visitors from unnecessary exposures to bloodborne
pathogens and other potentially infectious body fluids.
Three types:
1-Low grade disinfection:
Quaternary ammonium: Bactericidal effect.
used for low amount- blood spillage.
N
2-Intermediate grade disinfection:
Phenol and 70-90% alcohol ;Bactericidal and
Virucidal effect.
Used for low amount -blood spillage (less than 50ml).
3-High grade disinfection:
Formaldehyde ,Glutaraldehyde, Sodium hydrochlorite
, and hydrogen peroxide.
: Sporicidal ,Mycobactericidal, Fungicidal, and
bactericidal effect.
Used for: high blood spillage (more than 50ml), and
fungal decontamination.
NOSOCOMIAL INFECTION SURVEILLANCE:
The development of a surveillance is an essential first step
to identify local problems , and evaluate the effectiveness
of the infection control activity.
Objectives:
The purpose of surveillance program is to detect, record,
and report hospital acquired infection aiming to reduce
them and their costs.
N
2. Strategy of Surveillance:
A surveillance system must meet the following criteria:
Simplicity: to minimize costs and work load, and promote
unit participation by feedback.
Flexibility: to allow changes when appropriate.
Acceptability: Evaluated by ICC according to data analysis.
Consistency: use standardized definitions and methodology
Sensitivity.
Specificity.
Infection Control Committee:
1-Management
2-Epidemiologist
3-Physicians
4-Other health care workers(Laboratory, or Nurse).
5-Clinical microbiologist
6-Pharmacy
7-Central supply
8-Maintenance
Tasks (most important) of the committee
-To review and approve a yearly program of activity
for surveillance and prevention.
-To review epidemiological surveillance data and identify
areas for intervention.
Role of the physician:
1-Direct patient care using practices which minimize
infection.
2-Appropriate practice of hygiene:
(hand washing, and isolation).
3-Supporting the infection control team.
4-Protecting their own patients from other infected
patients and from hospital staff who may be infected.
5-Obtaining appropriate microbiological specimens when
an infection is present or suspected.