Negative Outcomes - Skin to Skin Contact
advertisement

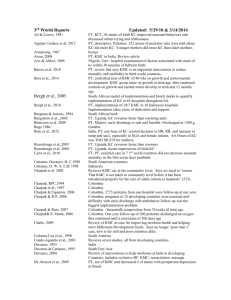
Negative Outcomes Update: 2/5/10 & 6/26/2012 Be sure to see Life Threatening chart for ALTES and Deaths in Birth KC Bauer, Pyper et al., 1998 Bauer J et al.,1996 Bohnhorst et al., 2001 27 weekers who got KC lost body temp. 28 or more weekers do not. 25-27 weekers lost body temp, 28 weeker or more do not. Proportion of regular breathing decreased in 2 nd hour of KC, possibly due to heat stress, even though temp in 2nd hour was still < 37.4 SSC is associated with an increased rate of bradycardia +desaturation/hr (a combined value) but no increase in bradycardias alone. Desats alone increased insignificantly during KC. Increased rate is not associated with overheating (pg. 500). “Increase in.brady + desat rate was not as great as in previous study because nurses made sure airway was unobstructed” (pg. 500). KC was associated with less regular breathing, probably due to brady + desat rate or parental movement interference (pg. 501). Mean axillary temp dropped 3/10 of a degree- due to no control over Insulation clothing across the infants’ backs. FT, descriptive of 7 neonatal deaths (5 in KC) over 5.5 years in France. PT, RCT, of KC early after birth and intermittent over next five days. Lower play/teaching NCAST score in KCs at 6 months. FT, infants who needed resuscitation while in Birth KC May be negative finding, will check it out??? Accidental extubation of one infant during ventilated KC 15 minutes of wriggling around when first put in KC with Substance abusing moms. PT, LBW, some mothers had problems adjusting to KMC but preferred it to incubator care. MATERNAL PROBLEM, not infant. PT, case study of one baby who desated during KC and did not in incubator. FT, reports what happened in Japan of death during birth KC FT/Late Preterm Cochrane concluded that “KC no apparent short- or long-term negative effects.” PT, RCT of early vs. late 24/7 KMC beginning within 24 hours of birth in stable premature infants. No difference in adverse events between the groups by discharge in Madagascar. FT, report of sudden infant death after Birth KC with full terms. FT, 2 case studies of apneic, hypotonic, pale infants at 5 and 70 mins post birth. Desaturations occur during transfer into/out of ventilated KC Recommendations for WHO to adopt related to KMC in NICU in developed countries and says that apnea, desats, and bradys with handling, routine care, or transfer into KC are obstacles to doing KMC. Recommendations from 7th INK meeting and says that instability is an obstacle to KMC PT, RCT, in India and 1 KMC and 5 controls died during study. PT, KMC is a risk factor for methicillin resistant staph aureus. Though no sig diff between groups, she goes on and on about how Temperature changes more than 0.1degree per hour and that is temperAture instability, and desats occur in 2nd hour of KC with BPD infants Though no sig diff between groups, she elaborates on how bad a 3 Point drop in low frequency HRV could be and that KC is stressful. Signal detection of apnea may be masked by maternal respiration if Electrode is on front of chest beneath mother instead of in infant axilla Suffocation by sleeping mothers of two babies and lack of good support From the slings in others. Bohnhorst et al., 2004 Bosque et al., 1995 Branger et al., 2007 Chiu & Anderson, 2009 Dageville et al., 2008 Diaz-Rosello et al., 1990 Drosten-Brooks,1993 Gale, Franck, Lund, 1993 Ibe et al., 2004 Jarrell et al., 2009 Mori et al., 2008/2009 Moore et al., 2012 Nagai, et al., 2010 Nakamura et al., 2007 Nakamura & Sano, 2008 Neu et al., 2000 Nyqvist, 2009 Nyqvist et al., 2009 Rao et al., 2008 Sakaki et al., 2009 Smith,2001 Smith 2002 Sontheimer et al.,1995 Van den Bosch& Nhaine, 1993 Visser et al., 2008 Wieland et al., 1995 PT, Descriptive of 23 preterms on 24/7 KMC ward in South Africa who got nosocomial RSV associated pneumonia due to inadequate infection control by staff and mothers. Of 167 first KC sessions of 30 minutes duration, KC had to be stopped for infant restlessness 5 times, for increasing apnea/bradycardia 4 times, for hypothermia 3 times, and for rapidly increasing FiO2 needs one time. Also, of 16 infants with elevated inspiratory oxygen need before KC, 13 infants needed more FiO2 during 30 minutes of KC (babies were 25-32 wk GA tested at 28 wks with wgts of 740-2125 grm with mean of 1110 gram on day 10 of life) .