Respiratory lecture notes
advertisement

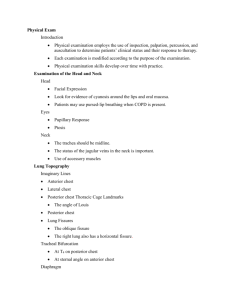
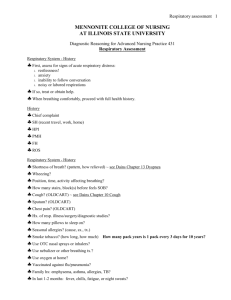
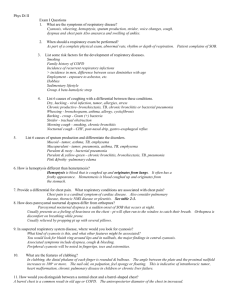
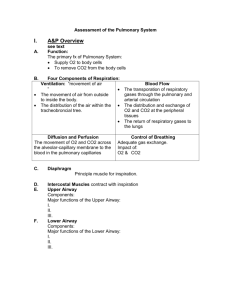
Page 1 of 4 Respiratory Assessment Components of Upper Airway Anatomy of the Thorax Trachea Lungs Diaphragm Pleura Parietal Visceral Mediastinum or interpleural space Bronchi Right Left Alveloli Lobes Right lung has three lobes Left lung has two lobes Thoracic Lines Muscles External intercostal muscles Accessory muscles Basic Clinical Assessment Patient History Inspection Palpation Percussion Auscultation Patient’s Respiratory History Cough Sputum production Dyspnea _________________________________ Chest pain Wheezing Subjective Questioning Are you having any trouble breathing? Do you have chest pain with breathing? Do you have a cough? Are you ever short of breath? Do you have problems breathing at night? Do you have any allergies? 1 Page 2 of 4 Do you smoke now or have you ever smoked? What kind of work did you do/did you do? Do you have a personal family hx of asthma, TB, lung CA, emphysema, or any other lung diseases? Considerations In Infants Respiratory distress Cyanosis Apnea SIDS in siblings Exposure to _________________________ Hx of prematurity or mechanical ventilation Night cough Swollen lymph nodes Sore throat or facial swelling Considerations in Older Adults Annual ______________________________ Recent changes in activity tolerance Change in number of pillows used at HS Significant weight change Night sweats Hand or leg swelling Inspection Patient Sitting Examine anterior and posterior chest Assess front, back and sides of chest Scars Wounds Lesions Symmetry of chest wall movement Inspiratory/expiratory cycles Respiratory pattern and breathing rhythm Other Considerations Sternocleidomastoid muscle Posture Scoliosis _______________________ Level of Consciousness (LOC) Confusion 02 therapy Respiratory Rates Infant 30 to 60 breaths per minute One year 20 to 40 “ 16 year 12 to 20 “ Adult 12 to 20 “ 2 Page 3 of 4 Abnormal Breathing Patterns Tachypnea Hyperpnea or Hyperventilation Kussmal breathing Bradypnea Cheyne-Stokes Ataxia Normal Inspection Findings Side to side symmetric chest shape Anterior-posterior diameter < transverse diameter Normal chest shape, with no visible deformities No muscle retractions when breathing Quiet, unlabored respirations without use of accessory muscles A regular respiratory rhythm Skin color that matches the rest of the body's complexion A respiratory rate of 12-20 in an adult Palpation Identify chest movement symmetry Chest skeletal abnormalities Tenderness Skin temperature changes Swelling and/or masses Trachea Placement Symmetry of Chest Expansion ______________________________ Normal Findings on Palpation Normal chest size and shape Warm, dry skin No tender spots Symmetrical chest expansion Tactile fremitus over the mainstem bronchi in front and between the scapulae in the back of the chest Percussion Produces sounds by tapping on the patient’s chest wall Sets chest wall and underlying tissues into motion Helps determine whether underlying tissues are filled with air, fluid, or solid material Work from Top Down Auscultation Listening to the sounds of the chest Breath sounds transmitted through the chest wall and through the diaphragm Assesses airflow through the tracheobronchial tree Not through clothing! ______________________ breaths through mouth Increases the duration, intensity, and thus detectability of any abnormal breath sounds that might be present 3 Page 4 of 4 Have the patient cough a few times prior to beginning auscultation. Clears airway secretions and opens small atelectatic (i.e. collapsed) areas at the lung bases. If the patient cannot sit up, auscultation can be performed while the patient is lying on their side. For those with respiratory conditions, start at posterior bases. Normal…Breath Sounds Chest Auscultation Listen for the sounds of normal breathing Listen for adventitious (added) sounds Anterior, Posterior, and Sides Modify based on pt Adventitious Breath Sounds Wheezing Crackles/Rales Stridor Pleural Friction Rub Documentation Example Anterior and posterior thorax appears symmetrical in a sitting and lying position. Respirations at 16, regular and effortless through nose. Breathing audible 1” from nose. No retractions, accessory muscle use, masses, nasal flaring, or visible superficial veins visible. Chest rise and fall of 1in. AP<T. No crepitus, masses, tenderness upon palpation. Thoracic expansion of <2 cm. Costal angle <90 degrees. Angle of ribs < 45 degrees. Breath sounds clear bilaterally in all lobes. No advantageous sounds. No assistive devices used. O2 stats 99% on room air.---------------------------------------------------------------------------------------------------------------------------John Smith ADNS Chippewa Valley Technical College 4