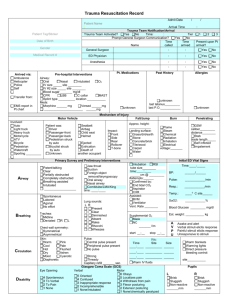
Scenario: Conscious multiple trauma patient
advertisement

Conscious multiple trauma patient
I.
Primary survey
1. Airway maintenance:
i.
ii.
iii.
iv.
v.
vi.
Can I request for some gloves please.
Stabilize the C-spine with collar and sand bags.
Do you remember what happened?
(Look in the airway for blood, vomitus, teeth or foreign bodies that
may obstruct the airway ).
Airway is patent.
(Feel for air coming in by placing hand over the mouth)
I can feel air.
(Place stethoscope on the neck)
There is breathing.
{If patient is unconscious – intubate.}
2. Breathing and ventilation:
a.
b.
c.
d.
e.
Do you feel any pain in your chest?
100 % oxygen by mask please.
(Look)
There are no wounds or bruising over the chest.
Patient has adequate respiratory movements.
There is no cyanosis.
Neck veins are not distended (or not visible if with collar).
(Feel)
There is no tenderness over the rib cage.
No crepitations.
Trachea is in the midline.
No flail segments.
(Listen over both sides at the axilla)
There is good air entry.
Breath sounds are symmetrical on both sides.
There is no stridor.
3. Circulation:
a.
b.
c.
d.
e.
f.
(Quickly assess the entire body for bleeding sites)
I am looking for any visible signs of external bleeding. There are none.
(Look at skin. Feel for distal pulses and proceed to more proximal pulses if
no pulses are detected at these sites. Press firmly over a nail bed until the
skin blanches then check for capillary refill. Normal: < 2 secs.)
Patient looks pale and his skin feels cold and clammy.
Peripheral pulses are weak. Capillary refill is slow.
Let us put the patient on monitor and can I please have the blood pressure,
pulse rate, and oxygen saturation checked every 5 mins.
If necessary, start I.V. resuscitation.
Insert 2 16 gauge IV lines, start NS 2L IV bolus
Draw blood for CBC, lytes, BUN, Creat, PT, PTT, INR
Type and cross match 6 U of blood
1
4. Disability
a. {Assess level of consciousness} Mr. Smith can you open your eyes?
A – Patient is alert…
V - responds to verbal stimuli…
P - responds to painful stimuli…
U - unresponsive
b. (Lift eyelids and shine light on each eye coming from the lateral side)
Mr. Smith I am going to shine a light in your eyes. Pupils are normal in
diameter, equal in size and reactive to light.
b. {Screen for C-spine injury}
Mr. Smith can you move your hands please….how about your feet.
There are no gross motor deficits.
5. Exposure
a. I would like to expose the patient fully.
b. Warm blankets please.
*The primary survey is interrupted to manage a life-threatening condition as soon as it is
detected. Once the condition is stabilized, the primary survey is continued. Should be done
rapidly and with a stable patient may take only 30 sec.
II. Take A.M.P.L.E. history
III. Secondary survey.
1. Complete head to toe survey.
a. Head
(Inspect and feel the head. Palpate the face and scalp.
Do a fundoscopy and otoscopy)
“There are no depressions, crepitus, lacerations.
No drainage from the ears or nose.
There is no bruising around the eyes or behind the ears.
Pupils are normal in size and equal and briskly reactive to light.
I would like to perform a fundoscopy.
No visible fluid on otoscopy. Tympanic membrane is intact.”
b. Neck
(Feel the cervical vertebra)
“There is no penetrating injury, bruising or tracheal deviation.
There are no palpable deformities or crepitations.
Does it hurt when I press?
c. Chest
(Inspect)
“There is no bruising or deformity. No flail segment.”
(Palpate the sternum, each rib and clavicle)
“Does it hurt when I press? There are no crepitations or tenderness.”
(Auscultate at apex, base and midaxillary areas)
“Heart sounds are clear. There is good air entry and symmetry.”
2
d. Abdomen
(Inspect)
There is no bruising or distention
(auscultate)
Bowel sounds are present.
(Palplate)
There is no guarding or tenderness.
e. Rectal
I would like to do a rectal exam.
2. Skeletal survey
a. Extremities
(Squeeze the bones of upper and lower extremities against each other with both
hands. Feel for peripheral pulses. Press down on the pelvis and press from the
sides like an accordion.)
“There are no swelling, deformity or tenderness. Pelvis is stable.”
b. (Inspect the back for injuries. Palpate the spine from the cervical vertebra to
the coccyx)
“I would like to log roll the patient on his side.
There are no visible deformities, wounds or bruising.
There are no tenderness, masses, or crepitations.”
3. Neurological
i.
ii.
iii.
iv.
v.
vi.
Perform GCS if px is unconscious
Press on forehead – look at eye opening
Press on forehead – listen to patient
Press on forehead – focus on movement
CN’s
a. III, IV, VI – follow my fingers w/ your eyes w/o moving
your head
b. V - can you feel this with your eyes closed
- corneal reflex (if unconscious)
c. VII – raise your eyebrows, show your teeth
d. IX, X – say ‘ah’
e. XI - can you lift your shoulders
f. XII – can you stick out your tongue
Motor
a. UE
b. LE
Muscle tone
- Flex and extend all 4 ext
Sensory
DTR’s
Cerebellar
vii.
.
4. I would like to insert a foley catheter (unless blood is present in the meatus), NGT.
5. I would also request for a CXR (AP),ECG, spine Xray (Lateral), pelvic Xray and
other necessary Xrays.
6. I would like to check the patient’s tetanus status.
3
Facial Trauma Checklist
Station:
A 27 y/o male, involved in a fistfight at a local bar was brought to ER. He is a known IV drug
abuser and a homosexual. You are the clerk on call. In the next 10 min. take a focused history
and conduct a focused exam relevant to the patient’s injury.
Hx:
Events of the accident
Use of weapons
Head injury
Loss of consciousness
Vomiting
Headache
Any visual problems (use of glasses/contact lenses)
Tetanus status
Allergies
Past Medical History
HIV status
Present Medications
P.E. :
Ask to wear gloves and mask
Indicates airway patency (ABC’s?)
Ask for vitals
Eyes:
Inspects the eye for swelling, contusion, lid laceration, subconjunctival
hemorrhage.
Examine pupils for size, reactivity and equality.
Evaluates visual acuity by counting fingers
(instruct patient to cover good eye and check bad eye
then examine and compare with the good eye with bad eye covered).
Assess extraocular muscle movement in all directions of gaze.
“do you notice any doubling of vision?”
Asks to perform a fundoscopy.
Face:
Inspects for and comments on facial asymmetry on facial/scalp
lacerations/contusions
Checks for bleeding into: oral cavity
both nares
both ears
Check for malocculsion
Palpates facial bones for tenderness and crepitus.
(maxilla, mandible, nasal, zygoma, orbital rim)
Palpate neck for tenderness.
Neuro: Test for facial sensation (CN V – V1-V2-V3-infraorbital)
Examine cranial nerves VII (facial)
Raise eyebrow, blow cheeks, shut eyes, etc.
Examines CNI (smell) by alcohol swab
Examine CN VIII (hearing) in the rt. Ear by tuning fork
Dx: blowout fracture of the infraorbital rim
Investigation: CT/MRI Rt. orbit
4
Hand Injury Checklist
History
1.
2.
3.
4.
5.
6.
7.
8.
9.
Orientation
Mechanism of injury
A.M.P.L.E. History
Reassurance
Mask, gown, gloves
Tetanus status
Handedness
Occupation/Hobbies
Previous History of Injury
Physical Exam
1. Inspect the dorsal and palmar aspects of the hand
(describe the wound: single/multiple, size, lacerations/abrasions, bleeding, foreign
body, clean/dirty, pale)
2. Palpate (check for tenderness, temperature)
3. Examine the range of motion of the hand and wrist by asking the patient to perform
these movements:
a. Test the flexor digitorum profundus
(support the patient’s proximal interphalangeal joint and ask patient to bend
fingers)
b. Test the flexor digitorum superficialis
(support the metacarpophalangeal joints and ask patient to bend fingers)
c. Bend the fingers forward at the metacarpophalangeal joint
d. Touch the thumb to each fingertip and make a fist
e. Spread the fingers apart and then touch them together
f. Bend the hand at the wrist up and down
4. Sensory :
Check on side of the laceration.
(“I would like to test your sense of touch.
With your eyes closed, tell me if I’m touching you with one or 2 ends of the wire”)
5. Vascular status
a. Capillary refill
Compare with normal hand
b. Check pulse if appropriate
5