Family Practitioner and HCV-Related Liver Disease
Prof. Eli Zuckerman, M.D.
Liver Unit
Haifa and Western Galilee District and
Carmel Medical Center
Clalit Health Services
Technion Faculty of Medicine, Haifa, Israel
מטרות השיעור
.1הכרת גורמי הסיכון למחלה
.2תפקיד רופא המשפחה באבחון המחלה
.3התייחסות רופא המשפחה לבני המשפחה (הדבקה ,כללי
התנהגות ,אמצעי זהירות ,הריון).
.4הטיפול ב ( : HCVרפואה מותאמת אישית ,2011חשיבות
ההקפדה על נטילת הטיפול ( ,)ADHERENCEתופעות
לוואי) .
.5תפקיד רופא המשפחה בטיפול
Diagnosis and screening
Prevalence HCV Infection in Israel
CHS ensured individuals: 3,926,182 (including
children)
Age >20 y/o: 2,658,885
Tested for HCV infection: 789,689 (20.1%)
age >20:
(29.7%)
18406 were HCV+: 2.3%
3067 died
prevalence 1.96%
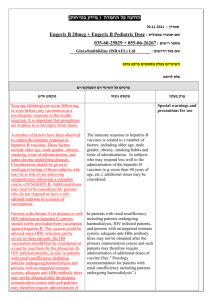
Seropositivity rate per 1,000, by country of birth - top 20 countries
(% of population tested) (14.7%-32.8%)
B razil
(17.4%)
Egypt
C anada
Italy
M o ro cco
(21.1%)
Lithuania
R o mania
Latvia
(30.5%)
B elarus
USSR
Kirghizstan
A zerbaijan
T ajikistan
(29.0%)
R ussia
Kazakhstan
Ukraine
Uzbekistan
M o ldo va
T urkmenistan
(29.5%)
Geo rgia
0
Hepatitis C from lab results, n=18,406
10/2010
10
20
30
seropositivity rate/1,000
40
50
60
Risk factors for HCV acquisition
Vertical transmission (perinatal): (2011)
Low risk (without HIV coinfection): 2-5%
No need for screening during pregnancy
No need for changing delivery approach
(i.e.Cesarean section)
Detection of HCV serology in the neonate
after 6-12 months.
Risk factors for HCV acquisition
Sexual transmission (2011)
Very rare if there is no HIV coinfection): 2-5%
Rare if no multiple sexual partners (> 5/year)
1 case per 1000 sex years
Considering non-traumatic sex and no
promiscuity: no need for protection.
Vandelli C, et al. Am J Gastroenterol. 2004;99:855-859
סיכום :מסקנות והנחיות לבני המשפחה
.1הריון :סיכון להדבקה נמוך.
אין הוראה לסקירה גורפת ל HCV
אין צורך בשינוי הגישה המHילדותית
בדיקת הילוד ל HCVרק לאחר שנה
.2אין צורך ב"בידוד" נשא של הנגיף (מגע ,אוכל ,ביגוד וכד')
טיפול בכפפות בפצע מדמם או מפריש.
.3הסיכוי להדבקה ביחסי מין בין בני זוג קבועים נמוך מאוד ולכן
אין צורך באמצעי הגנה (קונדום)
Whom to screen for HCV infection?
• Those who received blood products before 1991
• Injection drug users (alcoholics?)
• Hemodialysis patients
• Patients from endemic geographical regions
• HIV or HBV infected patients
• Screen for intra-familial transmission? (infants>1y, spause)
• Sexual promiscuity (MSP)
• Occupational exposure
• Piercing & tattooing
Ghany MG, et al. Hepatology. 2009;49:1335-1374.
Centers for Disease Control and Prevention. MMWR Recomm Rep. 1998;47:1-39.
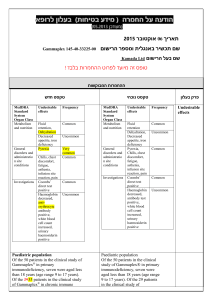
hepatocyte
Hepatitis,
Cirrhosis,HCC
HCV
lymphocyte
Autoimmune and
lymphoproliferative
disorders
Vasculitic purpura in a patient with HCV and
cryoglobulinemia
HCV Screening by the family practitioner
“Formal” risk factors including country of
origin
Abnormal liver tests (ALT and/or AST)
Extra-hepatic manifestations:
Arthritis/arthralgia (especially with RF+)
Raynould’s, peripheral neuropathy , fatigue
תפקיד רופא המשפחה בטיפול בחולים ב
HCV
.1הכרת גורמי הסיכון למחלה
.2תפקיד רופא המשפחה באבחון המחלה
.3התייחסות רופא המשפחה לבני המשפחה (הדבקה ,כללי
התנהגות ,אמצעי זהירות ,הריון).
.4הטיפול ב ( : HCVרפואה מותאמת אישית ,2011חשיבות
ההקפדה על נטילת הטיפול ( ,)ADHERENCEתופעות
לוואי) .
.5תפקיד רופא המשפחה בטיפול
Treatment
Treating chronic hepatitis C
10 years of progress
% sustained response
80%
72%
61%
60%
54%
34%
40%
41%
29%
16%
21%
20%
5%
0%
IFN 24w
IFN 48w
Peg 0.5
Peg 1.5
IFN-R 24w
IFN-R 48w
Peg-R
Optimal Peg-R
Optimal +
Adherence
Optimizing IFN Alfa Pharmacokinetics
Serum Levels
Higher-dose IFN
Optimized PK
Conventional IFN
Time
1 Week
Complete and sustained response
SVR
©Copyright Science Press Internet Services
Sustained Virologic Response
Primary Goal of Therapy
ANTI-VIRALTHERAPY
SVR is durable (99.6%)
secondary Goals:
Reduce HCV-RNA titer
Improvement of histology
Slow disease progression
Reduce risk for HCC
Hepatitis C: Immune-mediated disease.
Mechanism of HCV persistence
Infected
Hepatocyte
Ineffective
Clearance
of Infected
Hepatocytes
TNF
IFN
Class I MHC
CD8
Apoptosis
TCR
CD8
CTL
Sites of HCV Effects to
Promote Persistence
Treatment Options for Chronic HCV
TH
+
+
TC
-
Protease inhibitors
Polymerase inhibitors
NK
+
Interferon
alfa
TS
-
+
-
Anti-viral
therapy
Treatment of HCV with Peg-IFNα
and Ribavirin
Genotype 1
48 weeks SVR~50%
Genotype 2/3 24 weeks SVR 60-90%
MW Fried et al. N Eng J Med 2002; 347:975-982.
MP Manns et al. Lancet 2001; 358:958-965.
Treatment of chronic hepatitis C: Increasing
the response rate
• Correct host-related co-factors
• Improve tolerability:
– Manage side effects and toxicity
– Tailor length of treatment
• Retreat if former treatment failed
(non responders and relapsers
• Use additional, new drugs
Treatment of chronic hepatitis C: Increasing
the response rate
• Correct host-related co-factors
• Improve access/tolerability:
– Manage side effects and toxicity
– Tailor length of treatment
• Retreat if former treatment failed
(non responders and relapsers
• Use additional, new drugs
TREATMENT OF CHRONIC HCV
Poor Prognostic Factors
Viral Factors
Genotype 1
High viral load
Host Factors
Disease severity: cirrhosis, advanced fibrosis
Race: African Americans, Hispanic
Increased age
Metabolic factors: Obesity, Insulin resistance, Steatosis
Correctable
Factors
Other Co-morbidities (HIV, HBV co-infection)
Low adherence and compliance
Ribavirin dosage
Non-early Response
Effect of Weight Loss on Antiviral Response
32 treatment-naive GT 1
HCV patients with
metabolic syndrome
15 patients on
low-calorie diet:
10% ↓ in BMI
17 control patients
HOMA:
4.86-3.45
(P = .0018)
pegIFN alfa-2b + RBV
Response: 60.0%
Tarantino G, et al. Gut. 2006;55:585.
Response: 17.6%
Side Effects of Treatment
תסמונת דמויית שפעת
•
• חולשה ועייפות
• כאבי שרירים וכאבי פרקים
• חום וצמרמורת
כאבי ראש
גרד ותפרחת עורית
נשירת שער
אנמיה
ירידה בספירה לבנה ()WBC
ובטרומבוציטים ()PLT
בחילה ,חוסר תיאבון
תופעות אוטואימוניות
ירידה במשקל
תופעות פסיכיאטריות
שלשול
• דכאון ,עצבנות ,אי שקט
שיעול טורדני ,תסנינים ריאתיים
• הפרעות בשינה
הפרעות בבלוטת התריס
Side Effects of RBV Treatment
)אנמיה (תמס דם
השרית מומים בעובר
שעול טורדני
תפרחת וגרד
חוסר תיאבון ובחילה
REBETOL®. PDR®. 56th ed. 2002.
Chutaputti A. J Gastro-enterol Hepatol. 2000;15(suppl): E156-E163.
Epidemiology of Depression in
HCV-Infected Patients )cont’d(
Prevalence of Symptoms in HCV-Infected Patients
Patients (%)
100
86
80
74
70
70
68
Irritability
Depression
Mental
tiredness
Abdominal
pain
60
40
20
0
Physical
tiredness
Lang CA, et al. J Pain Sym Manage. 2006;31:335-344.
PegIFN Treatment-Associated Adverse Effects
Patients should be carefully monitored for adverse events
Most common adverse events: flu-like symptoms (fever, chills, headache,
malaise, and myalgia) as well as psychological impairment
Increase in
Incidence/Severity
Anemia
Neutropenia
Depression
Fatigue
Anxiety
0
1
2
3
Months
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2008;6:1315-1341.
4
Flu-like
symptoms
Treatment of chronic hepatitis C: Increasing
the response rate
• Correct host-related co-factors
• Improve access/tolerability:
– Manage side effects and toxicity
– Tailor length of treatment
• Retreat if former treatment failed
(non responders and relapsers
• Use additional, new drugs
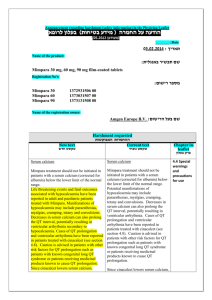
Management of common adverse effects of HCV
treatment with peg-IFN alpha and ribavirin
Adverse effect
“Flu-like” symptoms
(fever, myalgia, headache)
Depression
anemia
Dermatologic: rash, dry
skin, pruritus
Treatment
Comment
acetaminophen, NSAID
(possibly as prophylaxis)
4-6 hours after IFN
injection. May persist
over several days
Paroxetine (seroxat),
citalopram (cipramil)
IFN dose reduction (optional)
Psychiatric assessment
(mod-severe), careful
monitoring
ribavirin dose reduction,
erythropoeitin (EPO)
EPO: early-onset
anemia
chlorpheniramine (ahiston),
fexofenadine (telfast), topical
hydrating lotion, topical
corticosteroids
במי לא מטפלים?
מעל גיל 70
מחלת כבד מתקדמת (צהבת ,מיימת ,דמום מדליות ,אנצפלופתיה)
ירידה משמעותית בספירות הדם
(המוגלובין< 12גר ,%טסיות < /50,000מ"ל ,ניטרופילים< /1500מ"ל)
מחלה פסיכיאטרית פעילה
סוכרת לא מאוזנת
רגישות יתר לתרופה (אלרגיה לאינטרפרון אלפא או ריבוירין)
מחלת רקע משמעותית (ממאירות פעילה ,מחלת לב ,ריאות…).
חוסר הסכמה ,אלכוהוליזם או שימוש פעיל בסמים
נשים בהריון (ריבוירין)
HCV Epidemiology in Israel 2001-2010
% of HCV Treated with Anti-Viral therapy
Total: 1739 + 300 (clinical trials) = 2039
HCV + patients: 18,406
~ 30%-40% are not eligible for treatment
Actual estimated treatment rate: ~ 16%-18%
תפקיד רופא המשפחה :שיפור שיעור
המטופלים ב HCVע"י:
.1זיהוי מועמדים מתאימים לטיפול ,השלמת
הערכה מהירה ומלאה והפנייתם בהקדם
אפשרי למרפאת הכבד
.2הגברת המוטיבציה לטיפול
.3הורדת רמת החרדה מתופעות הלוואי של
הטיפול
.4מניעת סחבת בהתחלת הטיפול בחולים
המתאימים
שלבים בסקירה ,אבחון והערכת חולה עם HCVעל ידי רופא המשפחה
ערנות לגורמי סיכון כולל אורח חיים ,ארץ מוצא -ופרוצדורות
רפואיות בעבר :בדיקה סרולוגית ל (HCV-ANTIBODY( HCV
HCV-positive
HCV genotype and Viral load
(quantitative PCR), HBV markers, HIV
תפקודי כבד מלאים כולל
ספירת דם ותפקוד סינטטי ,
USכבד
HCV RNA not detected: repeat
HCV RNA within 6 months
הערכת התאמה לטיפול :גיל < ,70מחלות רקע
משמעותיות ,שימוש פעיל בסמיםו/או אלכוהול,
העדר ציטופניה משמעותית
שיחה עם החולה ומשפחתו על
צורך וחשיבות הטיפול
הפניה למרפאת כבד
Predictability
(news)
Time Course of Virological Response to IFN Therapy
in Patients with CHC
HCV RNA
100%
Lymphocyte
Induction phase
Maintenance phase
0%
1st dose
Detection limit
14–28 Days
?
Ferenci. Viral Hep Rev. 1999.
PEGASYS® (Peginterferon Alfa-2a [40KD]) Plus RBV:
Week 12 Predictability
Early Viral Response*
SVR
Yes
86%
Overall
(n = 390)
67%
(n = 261)
All patients
(N = 453)
No
14%
(n = 63)
NPV = 97%
3%
(n = 2)
*HCV RNA negative or drop of 2 log10 PCR.
Hoffmann-La Roche. Data on file. Updated from Fried MW. DDW Annual Meeting. 2001.
Therapy for Chronic Hepatitis C
HCV Genotype
Genotype 1 (4, 5, 6)
HCV-RNA Quantitative
at Week 12
≥2 Log Drop
Peginterferon alfa Plus
1.000-1.200 mg Ribavirin
for 48 Weeks
Genotype 2/3
Peginterferon alfa Plus
800 mg Ribavirin
for 24 Weeks
Treatment of chronic hepatitis C: Increasing
the response rate
• Correct host-related co-factors
• Improve access/tolerability:
– Manage side effects and toxicity
– Tailor length of treatment
• Retreat if former treatment failed
(non responders and relapsers
• Use additional, new drugs
CHRONIC HEPATITIS C
Types of Virologic Response
Peginterferon and Ribavirin
HCV-RNA (Log IU/mL)
7
6
NR: <2 log10 drop
5
Slow response: HCV-RNA negative Weeks 12-24
4
EVR: >2 log10 drop or negative
3
RVR: HCV-RNA negative
2
1
Undetectable
SVR
0
-8
-4
-2
0
4
8
12
16
20
24
32
40
Weeks After Start of Therapy
Davis G et al. Hepatology. 2003;38;645-652.
48
52
60
72
CHRONIC HEPATITIS C
Types of Virologic Response
Peginterferon and Ribavirin
HCV-RNA (Log IU/mL)
7
6
NR: <2 log10 drop
5
Slow response: HCV-RNA negative Weeks 12-24
4
EVR: >2 log10 drop or negative
3
RVR: HCV-RNA negative
2
1
Undetectable
SVR
0
-8
-4
-2
0
4
8
12
16
20
24
32
40
Weeks After Start of Therapy
Davis G et al. Hepatology. 2003;38;645-652.
48
52
60
72
CHRONIC HEPATITIS C
Types of Virologic Response
Peginterferon and Ribavirin
HCV-RNA (Log IU/mL)
7
6
5
4
RVR: HCV-RNA negative
3
2
1
Undetectable
SVR
0
-8
-4
-2
0
4
8
12
16
20
24
32
40
Weeks After Start of Therapy
Davis G et al. Hepatology. 2003;38;645-652.
48
52
60
72
Very high SVR rates with 24 weeks’ therapy in genotype 1 patients
with an RVR and LVL !!! (< 800,000 IU/ml)
SVR (%)
PEG-IFN α2a 180 g/wk plus ribavirin 1000/1200 mg/day
93%
96%
27
27
24 weeks
48 weeks
100
90
80
70
60
50
40
30
20
10
0
n=
RVR = HCV RNA <50 IU/mL at week 4
LVL (low viral load) ≤800 000 IU/mL;
HVL (high viral load) >800 000 IU/mL
Jensen D, et al. Hepatology 2006; 43: 954)
CHRONIC HEPATITIS C
Types of Virologic Response
Peginterferon and Ribavirin
HCV-RNA (Log IU/mL)
7
6
5
Slow response: HCV-RNA negative Weeks 12-24
4
3
2
1
Undetectable
SVR
0
-8
-4
-2
0
4
8
12
16
20
24
32
40
Weeks After Start of Therapy
Davis G et al. Hepatology. 2003;38;645-652.
48
52
60
72
SVR (%)
Consistent improvement with 72 weeks’ therapy
in G1 patients with a partial EVR
100
90
80
70
60
50
40
30
20
10
0
48 weeks
72 weeks
69%
52%
46%
44%
33%
16%
n=
46
46
31
25
25
16
Berg et al.
TeraVic-4
Ferenci et al.*
RBV 800 mg/day
RBV 800 mg/day
RBV 1000/1200 mg/day
partial EVR = no RVR and >2 log10 drop but
HCV RNA >50 IU/mL at week 12
* Includes small number (<10%) of G4 patients
Sánchez-Tapias JM, et al. APASL 2007; Abstract 0-196
TIME TO BECOME HCV RNA NEGATIVE
DURATION OF TREATMENT
RVR
cEVR
Slow to
Respond
4
12
24
48
WEEKS
72
TIME TO BECOME HCV RNA NEGATIVE
DURATION OF TREATMENT
RVR
cEVR
Slow to
Respond
4
12
24
48
WEEKS
72
TIME TO BECOME HCV RNA NEGATIVE
DURATION OF TREATMENT
RVR
cEVR
Slow to
Respond
4
12
24
48
WEEKS
72
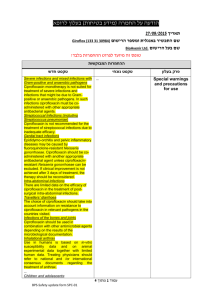
Proposed Algorithm for HCV genotype 1 patients
Quantitative PCR at baseline (-6m)
Start treatment
Viral load ≥ 400,000 IU/mL
RVR
24 weeks
treatment
No RVR
48 weeks
treatment
TestHCV
for ETR
RNAat
week
24 12
at week
HCV RNA
at week 12
Test for ETR at
week 24
Test for ETR
at week 48
Test for SVR
at week 48
Viral load > 400,000 IU/mL
Test for SVR
at week 72
Week 12 HCV RNA
≥-2 log
negative
48 weeks
treatment
Week 24 HCV RNA
+
72 weeks
treatment
≥-2 log
Stop
Optimising outcomes
in genotype 2/3
SVR Rates in Genotype 2/3 Patients Achieving RVR
With Shorter Duration Tx
RVR Patients Treated With PegIFN alfa-2a + Weight-Based RBV[1,2]
Von Wagner et al[2]
100
100
82
80
80
SVR (%)
80
SVR (%)
Shiffman et al[2]
60
40
85*
60
40
20
20
0
0
16 Wks
(n = 71)
79
24 Wks
(n = 71)
*P = .002 vs 16 wks.
1. Von Wagner M, et al. Gastroenterology. 2005;129:522-527.
2. Shiffman M, et al. N Engl J Med. 2007;357:124-134.
24 Wks
16 Wks
(n = 733) (n = 732)
Proposed Algorithm for HCV genotype 2/3 patients
Quantitative PCR at baseline (-6m)
Start treatment
Viral load ≥ 400,000 IU/mL
No significant fibrosis
RVR
16 weeks
treatment
Test for ETR at
week 16
Test for SVR
at week 40
Viral load > 400,000 IU/mL
significant fibrosis
No RVR
24 weeks
treatment
24 weeks
treatment
Test for ETR at
week 24
Test for SVR
at week 48
Suboptimal Virologic Responses
HCV RNA (log10 IU/mL)
8
PegIFN/RBV
7
6
5
4
Relapse
Null response
Partial
response
Breakthrough
2 log10 decline
3
2
Limit of detection
1
0
0 4 8 12 18 24 30 36 42 48 54 60 66 72 78
Wks
Impact of Prior Type of Therapy and Response on
SVR Overall
EPIC3: Proportion of Patients Achieving SVR
PEG-IFN alfa-2b (1.5 µg/kg/wk) + Ribavirin (800–1400 mg/d) , 48 weeks
100
90
80
70
60
50
40
30
20
10
0
Nonresponder
Relapser
43%
34%
32%
18%
7%
IFN/RBV
(n = 1203)
PEG2b/RBV
(n = 460)
Poynard T et al. EASL 2008, EPIC3. Abstract 988., Oral Presentation.
6%
PEG2a/RBV
(n = 360)
Similar SVR Across All Previous Response
Histories in Patients HCV RNA Negative at Week 12
Retreatment with PEG-IFN alfa-2b (1.5 µg/kg/wk) + Ribavirin
(800–1400 mg/d) 48 weeks
% of Patients
100%
80%
56%
54%
60%
40%
20%
0%
Relapsers
Data on File, Schering-Plough Corporation.
Nonresponders
Treating chronic hepatitis C
10 years of progress
Optimal adherence
% sustained response
80%
72%
61%
60%
54%
34%
40%
41%
29%
16%
21%
20%
5%
0%
IFN 24w
IFN 48w
Peg 0.5
Peg 1.5
IFN-R 24w
IFN-R 48w
Peg-R
Optimal Peg-R
Optimal +
Adherence
Adherence to Full Course Treatment
Impacts SVR Overall — The 80/80/80 Rule
SVR Stratified by Time on Therapy and Adherence:
≥ 80% PegIFN Dose, ≥ 80% RBV Dose, ≥ 80% of the Time
70%
60%
62%
50%
51%
40%
30%
34%
20%
10%
0%
Always
First 12 Weeks Only
Never
JG McHutchison et al. Gastroenterology 2002
© 2006 SCHERING-PLOUGH
Enhancing Response
Patient
Selection
Prescribe
PEG IFN
and RBV
Provide best
support and
education
Facilitate
Adherence
Response
Monitor
side effects
Evaluate early
response
Manage side effects
via dose reduction
rather than
discontinuation
תפקיד רופא המשפחה בטיפול ב HCV
הסבר על מהות הטיפול ,חשיבותו ,תופעות הלוואי
הצפויות.
הדגשת החשיבות של נטילה רציפה ומלאה של הטיפול
בהשגת תגובה וירולוגית.
פיקוח ומעקב על נטילה רציפה ונכונה (על פי מרשמי
תרופות ושיחה תכופה עם החולה ומשפחתו)
שיתוף המשפחה בתמיכה בחולה בזמן הטיפול ובתופעות
הלוואי הצפויות
תפקיד רופא המשפחה בטיפול ב HCV
ערנות להופעת תופעות לוואי (במיוחד פסיכיאטריות) וזיהוי
שינוי במצב הרוח ,הפרעות שינה ,אי שקט ,עצבנות ודיכאון
בשלב מוקדם .טיפול תרופתי וגיוס המשפחה לתמיכה
במקרים קלים בשלב מוקדם .הפניה למומחים ספציפיים
(פסיכיאטר ,דרמטולוג) במקרים הקשים תוך תיאום ודווח
למרפאת הכבד המטפלת.
ביצוע בדיקות מעקב החורגות מהפרוטוקול במקרה של
תופעות לוואי
תיאום ושיתוף פעולה במעקב וטיפול עם הגורמים
המטפלים :אחות המרפאה ,עובד(ת) סוציאלי(ת) ,מרפאת
הכבד ,מומחים שונים
SNP rs12979860: distribution and SVR
African Americans
Clark PJ et al. A J Gastroenterology, 2010
Caucasians
Consideration for Treatment in 2011
Likelihood of response to IFN + RBV
• Naive vs treatment experienced
• HCV genotype
• HCV RNA level
• Race
• IL28B type
Likelihood of disease progression
• Histologic staging
Likelihood of tolerating IFN + RBV
סיכום ומסקנות“Take –home :
”message
לערנות ופעולת רופא המשפחה חשיבות מכרעת בזיהוי גורמי סיכון
לזיהום ב ,HCVאיתור החולים וביצוע בדיקות סקירה ל HCV
לחולים בסיכון.
באחריות רופא המשפחה ביצוע הערכה ראשונית של תפקודי כבד,
הערכת מדדים וירולוגים ובחירת חולים מתאימים לטיפול.
הטיפול ב HCVממושך וכרוך בתופעות לוואי המשפיעות על התפקוד
ואיכות החיים אך מאידך עשוי להביא להחלמה מלאה מהזיהום
הנגיפי ברוב המקרים.
השגת SVRמביאה לשיפור היסטולוגי ,האטה בהתקדמות המחלה
(במקרה של פיברוזיס מתקדם) ירידה בשיעור הסיבוכים ובשיעור
הופעת HCCבחולים עם צירוזיס.
סיכום ומסקנות“Take –home :
”message
ההחלטה הטיפולית מתבססת על מספר פרמטרים הכוללים את גיל
החולה ,מחלות רקע ,הגנוטיפ הויראלי ,העומס הנגיפי ,חומרת מחלת
הכבד ,ובעתיד הקרוב קביעת פולימורפיזם גנטי ל.IL28B -
הטיפול האנטי ויראלי הינו טיפול מותאם אישית ומבוסס על הגנוטיפ
הויראלי והתגובה הוירולוגית המוקדמת תוך כדי הטיפול.
לרופא המשפחה חשיבות מכרעת בפקוח על נטילה רציפה ומלאה
של הטיפול התרופתי ( ,)adherenceהקשורה בהשגת ,SVRעידוד
ותמיכה בחולה בזמן הטיפול ובזיהוי וטיפול בתופעות לוואי בשלב
מוקדם.
ההצלחה בטיפול תלויה בשיתוף פעולה בין גורמים רבים הכוללים את
החולה ומשפחתו ,אחות המרפאה ,עו"ס ,רופא המשפחה ,מרפאת
הכבד המטפלת ומומחים בתחומים הרלבנטיים לסיוע בתופעות
הלוואי הקשורות לטיפול .לתיאום מוצלח בין כל הגורמים באמצעות
רופא המשפחה חשיבות מכרעת בהצלחת הטיפול.