Welcome to N 152
Diffusion
• The tendency of a molecule to move
from a region of high concentration to
one of lower concentration. Can be
altered by:
– The partial pressure gradient of the gases
– The thickness of the respiratory membrane
– Pressure in the pulmonary circulation
– Surface area available
Perfusion
• The flow of blood that supplies tissues
and cells with needed nutrients and
oxygen
Chemoreceptor control of
respirations
• Groups of nerve cells that can distinguish
between hydrogen ions and oxygen
• Exert greatest influence on the autonomic
nervous system’s control of ventilation by
correlating acid-base balance with gas
exchange requirements
• Located both centrally and peripherally
(carotid arteries and arch of the aorta)
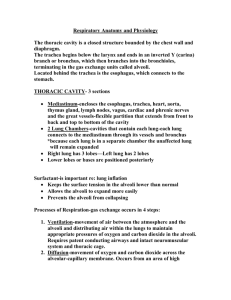
Anterior Landmarks
Posterior Landmarks
Lateral Landmarks
History
• HPI
– Current symptoms
– Chief complaint
•
•
•
•
•
•
•
Dyspnea
Cough
Sputum production
Hemoptysis
Wheezing, stridor
Chest pain
Cyanosis
Ability to Breath
•
•
•
•
Respiratory Rate
Minute ventilation
Vital capacity
Inspiratory force
Chest Diameter
Chest Abnormalities
Percussion Notes
•
•
•
•
•
Resonance
Hyperresonance
Dull
Flat
Tympany
Normal Breath Sounds
Adventitious Breath Sounds
•
•
•
•
Crackles
Rhonchi
Wheezes
Pleural Friction Rub
Normal V/Q
Low V/Q
High V/Q
Silent Unit
Lung Volume Tests
• Tidal Volume (VT)
– The volume of air inspired and expired during the
respiratory cycle. 5-8 ml/kg
• Inspiratory Reserve Volume (IRV)
– The maximal amount of air that can be inspired
after a normal inspiration
• Expiratory Reserve Volume (ERV)
– The maximal amount of air that can be expired
after a normal inspiration
• Residual Volume (RV)
– The volume of air remaining in the lungs at the
end of maximum expiration
Peak Flow Meters
Lung Capacity Tests
• Functional Residual Capacity (FRC)
– The volume of air remaining in the lungs at the
end of normal expiration. Calculated
measurement of of airway resistance.
• Vital Capacity (VC)
– The maximum amount of air that can be expired
slowly and completely after a maximum inspiration
• Total Lung Capacity (TLC)
– The volume of air contained in the lung after
maximal inspiration
Pulmonary Spirometry Tests
• Forced Vital Capacity (FVC)
– The volume of air expired forcefully and
rapidly after maximal inspiration
– Measured over over a specific interval of
time
• Peak Expiratory Flow Rate (PEFR)
– The maximum flow rate attainable at the
beginning of forced expiration
Obstructive Disorders
• Increased resistance to airflow
– Emphysema, asthma, chronic bronchitis,
bronchiectasis
•
•
•
•
•
VC
TLC
FRC
RV
FEV1
Restrictive Disorders
• Compliance of lungs, chest wall, or both
– Neuromuscular diseases: polio, MD,
kyphoscoliosis, chest wall abnormalities
•
•
•
•
•
VC
TLC
Normal FRC
Normal RV
FEV1
Arterial Blood Gases
• pH:
7.35 – 7.45
• PCO2:
35 – 45 mm Hg
• HCO3: 22-26 mEq
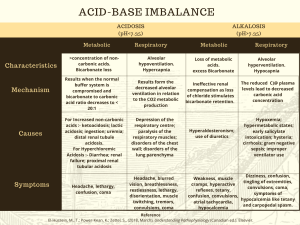
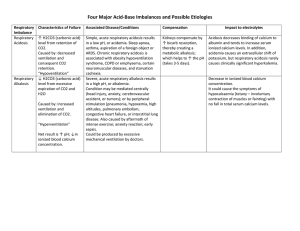
General Imbalances
• Acidosis:
< 7.35
– An accumulation of either acids or a loss of
bicarbonate
• Alkalosis:
> 7.45
– An accumulation of base or a loss of acids
Respiratory Acidosis
• Etiology: hypoventilation
• Causes: pain, drugs, neuromuscular
disorders, obstructive/restrictive lung
diseases, respiratory center depression,
fatigue, mechanical hypoventilation
• Sx: decreased mental status, drowsiness,
restlessness, tachycardia, hypoventilation,
headache, weakness, tremors
Respiratory Acidosis (cont)
• Non Invasive Treatment
– Voluntary deep breathing
– IPPB
– Incentive devices
– Pain medication
• Invasive Treatment
– Artificial airway
– Mechanical ventilation
Respiratory Alkalosis
• Etiology: hyperventilation
• Causes: anxiety, fear, pain, fever,
sepsis, brain lesion, hypoxia, exercise,
mechanical hyperventilation
• Sx: increased respiratory rate,
increased tidal volume, cramps, tetany,
paresthesias, seizures
Respiratory Alkalosis (cont)
• Treatment:
– Reassurance
– Sedation
– Pain medication
– Rebreathe CO2
– Reduce ventilator settings to decrease RR
and tidal volume
Metabolic Acidosis
• Loss of Base
–
–
–
–
Diarrhea
Pancreatic drainage
Renal disease
Fistula
• Increased Acids
–
–
–
–
–
DKA
Salicylate overdose
Sepsis/lactic acidosis
Renal failure
starvation
Metabolic Acidosis (cont)
• Sx: decreased mental status, confusio,
seizures, fatigue, drowsiness,
hypotension, anorexia, vomiting,
nausea
• Treatment
– Treat the underlying cause
– In severe cases, Sodium Bicarbonate may
be ordered
Metabolic Alkalosis
• Increase Base
– Sodium Bicarbonate administration
– Ingestion of alkaloids
• Decreased Acids
– Vomiting
– NG tube suctioning
– Electrolyte imbalance
Metabolic Alkalosis (cont)
• Treatment
– Treat the underlying cause
– Administer acid (ammonium clloride
– Increase bicarbonate excretion with
Diamox
– In severe cases, dialysis may be ordered
Bronchoscopy
Thoracentesis
 0
0