Parkinson`s Disease (PD) and Treatment
advertisement
 and Treatment")
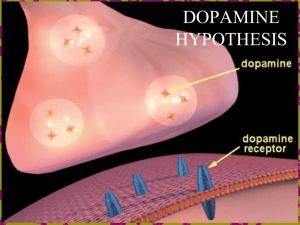
Jieun Park Chem-5398 Outline Overview Diagnosis Treatment Physical Therapy Drug Therapy Surgery New Research 2 Overview Second most common human neurodegenerative disorder. Prevalence of 1 out 272 in U.S. Increases to 4 to 5% for ages 85 and over. Degeneration of dopaminergic neurons in the substantia nigra. Dopamine 3 Overview cont’d Symptoms caused by insufficient dopamine. 3 main symptoms: Tremors Rigidity Slowed motion (Bradykinesia) Other symptoms include: Dementia, sleep disturbances, depression, etc. 4 Overview cont’d Common cause of chronic progressive parkinsonism. Exact causes still yet unknown. Gene mutation Toxins Trauma 5 Diagnosis No definitive tests for PD. PET scans can aid to determine levels of dopamine. Difficult to diagnose, many symptoms shared with other disorders. Medical history and neurological tests are conducted to diagnose. Usually, if two of the cardinal symptoms are present. 6 Treatment – Parkinson’s Disease No cure for PD. Treatment can be divided into two stages. Early and Later stages Early stage Onset of symptoms, treated with physical therapy and medications (Levodopa, dopamine agonists, etc) Later stage Usually after having received 5+ years of levodopa treatment. “Wearing-off” and “On/Off” effect develops, other medication in conjunction levodopa is commenced. MAO-B and COMT inhibitors. 7 Treatment – Physical Therapy Regular exercise Recommended throughout the life of disorder. Helps maintain and improve mobility and strength. Physical exercise aids in rigidity relief, muscle strength and flexibility, balance, etc. Caution is advised to avoid sudden movements or strenuous activities – fall could result in serious injury. 8 Treatment – Drug Therapy Levodopa (L-DOPA) Preferred medication to control major symptoms. Usually administered at the early onset of disorder. Drug is well tolerated and side affects are limited. Levodopa Dopamine 9 Drug Therapy – L-DOPA L-DOPA is converted to Dopamine by enzyme DOPA decarboxylase (DDC). 10 Drug Therapy – L-DOPA Used with Carbidopa, which blocks the early conversion of L-DOPA into dopamine. Carbidopa 11 Drug Therapy – L-DOPA 12 Drug Therapy – L-DOPA Side effects include Psychiatric symptoms; linked to depression Nausea and vomiting Prolonged use can cause “wearing-off” effect. Leads to other motor complications, such as dyskinesia. Still the preferred treatment for symptoms. Drug brand name: Sinemet ® 13 Drug Therapy – L-DOPA L-DOPA can cross blood-brain barrier, when dopamine cannot. This led to the idea of using L-DOPA as treatment for PD. First used in the 1960’s, with daily increase dosage program. L-DOPA used in combination with Carbidopa in 1967. Increases potency of L-DOPA up to 4-fold. 14 Treatment – Drug Therapy Dopamine Agonists Acts directly on the dopamine receptors. Initially was used with L-DOPA. Today, sometimes prescribed before L- DOPA, to delay “wearing-off” effect and other motor complications brought on by prolonged use of L-DOPA. Pramipexole Dopamine 15 Drug Therapy - DOPA agonists Triggers dopamine receptors in place of depleted dopamine neurotransmitters. http://www.youtube.com/watch?v=dTdW8q9hukw&feature=related 16 Drug Therapy – DOPA agonists Adverse side effects Nausea, dizziness, hallucinations Sleep attacks, hypotension Permax ® (pergolide) pulled after direct link to fibrosis of cardiac valves that can lead to death. Unavailable in U.S. since 2007. 17 Treatment – Drug Therapy Monoamine Oxidase B (MAOB) Inhibitors Delays or reduces breakdown of dopamine by MAO-B. Used as monotherapy or in conjunction with L-DOPA, it can reduce the dosage of L-DOPA by 15%. Selegeline 18 Drug therapy – MAO-B Inhibitors MAO-B is an enzyme that metabolizes dopamine. From the breakdown of dopamine, hydrogen peroxide is produced, which the oxidative stress can damage dopaminergic neurons in the substantia nigra. (Possibly neuroprotective) MAO-B inhibitor delays or reduces the metabolism of dopamine. 19 20 Drug therapy – MAO-B Inhibitors Side effects of L-DOPA may be enhanced by selegeline. Nausea and dizziness. 21 Treatment – Drug Therapy Catechol O-Methyl Transferase (COMT) Inhibitors Inactivates and degrades neurotransmitters, such as dopamine. Mainly used in combination with L-DOPA, it increases the half-life of L-DOPA. Delays “wearing-off” effect of L-DOPA and other motor complications such as dyskinesia Tolcapone(Tasmar ®) 22 Drug therapy – COMT Inhibitors COMT catalyses methylation of L-DOPA. Addition of COMT inhibitor along with LDOPA and carbidopa prolongs the half-life of L-DOPA and increases the amount in the CNS. This increases “on” time for L-DOPA. Tasmar ® are hepatotoxic. Diarrhea and sleep disturbances 23 Treatment – Drug Therapy Amantadine Antiviral agent. Known to aid in reducing dyskinesia. Anticholinergics Improve tremors and stiffness Cause impairment and constipation 24 Treatment - Surgery Before commerciality of levodopa, surgical treatment were preferred. Early surgeries were successful with tremors, but failed to relieve other symptoms. “Means of last resort” due to high risk of potential complications. Recent advances in neurosurgical procedures allow for better treatment. 25 Surgery Deep Brain Stimulation Brain pacemaker, sends electrical impulses to brain to stimulate the subthalamic nucleus. Improves motor functions and reduce motor complications. Complications include: brain hemorrhage, seizures, death. 26 New Researches Nicotine Intake of nicotine has shown to slow the degeneration of neurons. Acts similar to levodopa. Melatonin Serotonin derivative that helps insomnia. Also shown to cause a reduction in production of neurodegenerative radicals. 27 Assigned Reading Jankovic, Joseph; Aguilar, L. Giselle. Current approaches to the treatment of Parkinson's disease. Neuropsychiatric Disease and Treatment (2008), 4(4), 743-757. 28 Homework Problems 1. 2. 3. Which medicinal treatment is generally started for younger patients with mild symptoms in early-stage treatment? Levodopa is used with which drug and why? Describe “wearing-off” and “on-off” effect. 29 References Davie, C. A. “A review of Parkinson’s disease”, British Medical Bulletin, 86 (2008): 109-127 Munchau, A., Bhatia, K P. “Pharmacological treatment of Parkinson’s disease”, Postgrad Med J, 76 (2000): 602-610 Rao, Shobha A., Hoffman, Laura A., Shakil, Amer. “Parkinson’s Disease: Diagnosis and Treatment.”, American Family Physician, 74 (2006): 2046-2054 Singh, N., Pillay, V., Choonara, Y. E. “Advances in the treatment of Parkinson’s disease”, Progress in Neurobiology, 81 (2007): 29-44 Images from Wikipedia, Google 30