PowerPoint Slides
advertisement

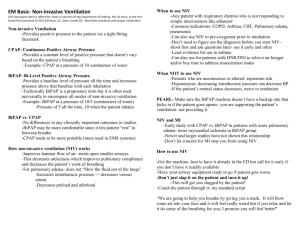
Nebulization during spontaneous breathing, CPAP and Bilevel: a randomized analysis of pulmonary radioaerosol deposition RESPIRATORY CARE APRIL 2014 VOL 59 NO 4 Douglas S. Gardenhire, EdD, RRT-NPS, FAARC Georgia State University Background • What do we know about aerosol and noninvasive ventilation? • No guidelines exist for aerosol delivery with noninvasive ventilation. • Small number of studies exist in topic. • Large number of variables encountered. • As a practicing respiratory therapist what variables do you think play a role in delivering aerosol to patients receiving CPAP or BiPAP? Background • What is scintigraphy? • What is technetium? Research Question Does pulmonary regional deposition of radioaerosol administered by nebulization to healthy individuals, during spontaneous breathing, CPAP and BiPAP differ? • Is this research question relevant to your clinical practice? Methods • Study design – Crossover and Observational – What are the positives to this design? Negative? • Exclusion criteria were: – – – – – – – – – – < 18 or > 60 years History of smoking History of respiratory diseases (COPD, asthma or tuberculosis) History cardiac disease Pregnancy Conditions requiring systemic corticosteroids, FEF1 < 2 L peak expiratory flow < 300 Liters/min BMI > 30 Kg/m2 Neuromuscular disease diagnosis or maximal inspiratory pressure (MIP) > -30 cmH2O. Methods (Cont.) • Control group was each patient. • Sample size small. • Do you see these as issues with the study? Methods (Cont.) Do you think the statistical analysis is appropriate for this observational study? • No ethical concerns noted for this paper. Results • Main results – Statistically no difference between spontaneous breathing, CPAP and BiPAP when using a jet nebulizer. – Why are they not different? Results (cont.) Results (cont.) • Why do you think the researchers found more aerosol in the stomach with BiPAP? Discussion • What do these finding mean to you as a respiratory therapist using CPAP and BiPAP? • The current study was very similar to: França EET, Andrade AFD, Cabrala G, Filho PA, Silva KC, Filho VCG, et al. Nebulization associated with Bi-level noninvasive ventilation: analysis of pulmonary radioaerosol deposition. Respir Med 2006;100:721-728. • Franca, et al. found a decrease in aerosol when using BiPAP in healthy volunteers. Discussion (cont.) • How does albuterol behave with the use of BiPAP in mild to moderate asthma? Pollack CV Jr, Fleisch KB, Dowsey K. Treatment of acute bronchospasm with beta-adrenergic agonist aerosols delivered by a nasal bilevel positive airway pressure circuit. Ann Emerg Med 1995;26(5):552–557. • Pollack et al. found an improvement in peak flows of asthmatics when using BiPAP. Discussion (cont.) • How does bronchodilator behave with the use of BiPAP in moderate to severe asthma? Galindo-Filho VC, Dornelas-de-Andrade A, Brandão DC, de Cássia S, Ferreira R, Menezes MJ, et al. Noninvasive ventilation coupled with nebulization during asthma crises: A randomized controlled trial. Resp Care 2013;58(2):241-249. • Deposition did not change, but patient outcomes improved via PFT values. • Could pressure differences make a difference? Discussion (cont.) • What additional work is needed in this area? – More is needed. More clinical evaluations. – Bench work is also important. – Cost may play a factor. Conclusions • Authors’ conclusions… – Aerosol deposition is equivalent in healthy volunteers during spontaneous breathing, CPAP and BiPAP. • Should this affect your practice? • Take-home message….. – Aerosol can be given during CPAP and BiPAP – Evaluate patients – Be consistent