Understanding Basic EKG - Weebly
advertisement

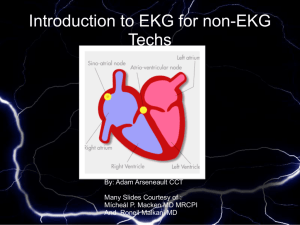
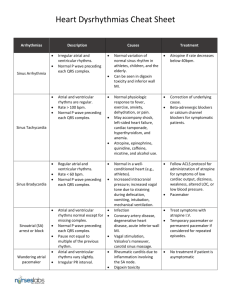
Zabrina Bellina University of Central Florida Teaching With Technology Project At the conclusion of this presentation, students will able to: 1. Describe coronary circulation and gain working knowledge of blood supply to heart structures. 2. Define the term electrocardiography and describe the electrical conduction system of the heart. 3. Correlate electrical events in the heart with the waveform represented in a normal EKG. 3. Gain understanding of EKG interpretation through waveform measurement, analysis, and correct rate computation of rhythm strips. 4. Understand and identify lethal cardiac arrhythmia waveforms. Figure 1 Superior & Inferior Vena Cava Right Atrium Tricuspid Valve Right Ventricle Pulmonary Semi-lunar Valve Pulmonary Trunk Right & Left Pulmonary Arteries Lungs Pulmonary Veins Left Atrium Mitral Valve Left Ventricle Aortic Semi-lunar Valve Aorta Body supplies blood to: Right Atrium Right Ventricle the SA Node in 55% of population the LV inferior wall the LV posterior wall and ⅓ of the posterior interventricular septum in 90% of the population supplies blood to: the Left Atrium the LV lateral wall the SA Node in 45% of the population and to the LV posterior wall ⅓ of the interventricular septum AV Node and Bundle of His in 10% of the population supplies blood to: the LV anterior and lateral walls the Left and Right Bundle Branches the anterior ⅔ of the interventricular septum Remember: The Right Coronary Artery supplies both the Right and Left heart. The Left Coronary Artery and its branches only supply the Left heart. An electrocardiogram (ECG) , also known as an EKG, is a graphic recording of the electrical activity of the heart. It is used as a diagnostic tool to assess cardiac function. An EKG is a painless procedure that can be performed by placing disposable electrodes on the skin of a person’s chest wall, upper and lower extremities. Figure 2 Figure 3 An EKG can be recorded with 12, 15, and sometimes even 18 leads. However, the 12 lead EKG is the most commonly used tool to diagnose cardiac conduction abnormalities, arrhythmias, myocardial infarction and ischemia. Remember, an EKG represents the electrical impulses that the heart transmits and are recorded as tracings on specialized graph paper. The Conduction System of the Heart Figure 4 The SA Node is the primary pacemaker for the heart at 60-100 beats/minute The AV Node is the “back-up” pacemaker of the heart at 40-60 beats/ minute The Ventricles (bundle branches & Purkinje fibers) are the last resort and maintain an intrinsic rate of only 20-40 beats/minute Let’s look at a normal conduction pathway: SA Node Myocardial Contraction AV Node Purkinje Fibers Bundle of His Right and Left Bundle Branches Myocardial Cells = the mechanical cells of the heart. They contract when they receive an electrical impulse from the pacemaker cells. Myocardial = Muscle (Brawn) Pacemaker Cells are very small cells within the conduction system which spontaneously generate electrical impulses. Pacemaker = Power Source (Brain) Electrical Conducting Cells rapidly carry current to all areas of the heart. Conducting Cells = Hard Wiring of Heart (Fuel) Now, let’s correlate the mechanical activity with the electrical activity…. Ventricular Systole Atrial Systole Ventricles repolarize Atria depolarize Figure 5 Ventricles depolarize Depolarization occurs when sodium channels open fast and the inside of the membrane becomes less negative (electrical stimulation). This is manifested as the P wave on an EKG, which signifies atrial muscle depolarization. The plateau that immediately follows the P wave represents atrial systole, when calcium channels open slowly and potassium channels close (at this time mechanical contraction of the atria takes place). The PR interval on an EKG reflects conduction of an electrical impulse from the SA node through the AV node. PR = 0.12 – 0.20 seconds Figure 6 The QRS complex of an EKG reflects ventricular muscle depolarization (the electrical impulse moves through the Bundle of His, the left and right bundle branches and Purkinje fibers). QRS = 0.08 – 0.10 seconds The QT interval measures the time from the start of ventricular depolarization to the end of ventricular repolarization. QT interval = < 0.43 seconds or ½ of the R-to-R interval The ST segment reflects the early ventricular repolarization and lasts from the end of the QRS complex to the beginning of the T wave. The T-wave on an EKG reflects ventricular muscle repolarization (when the cells regain a negative charge - the “resting state”) and mechanical relaxation, which is also known as diastole. Keep in mind how electricity flows… When an electrical current moves toward a positive electrode, the deflection on the EKG strip will be positive (up). When an electrical current moves toward a negative electrode, the deflection on the EKG strip will be negative(down). ST Segment Changes Any elevation in the ST segment that is greater than two small boxes is indicative of myocardial injury. Any ST segment depression greater than two small boxes indicates myocardial ischemia. EKG paper comes in a roll of graph paper consisting of horizontal and vertical light and dark lines. The horizontal axis measures time Figure 7 The vertical axis measures voltage One small square = 0.04 seconds One large square = 0.2 seconds or One small square(0.04) x 5 The light lines circumscribe small squares of 1 x 1 mm One small square = 0.1 mV The dark lines delineate large squares of 5 x 5 mm One large square = 0.5 mV Rhythm Rate P - waves PR Interval QRS Complex Rate What’s the normal heart rate for an adult human being? 60 – 100 beats/ minute Is the rate in your strip too fast or too slow? In terms of rate computation, heart rate generally refers to the number of ventricular contractions that occur in 60 seconds or one minute. When calculating rates, if there is a P-wave in front of every R-wave, the atrial and ventricular rates will be the same. . Atrial rate can be calculated by measuring the interval of time between P-waves (the P-to-P intervals). Ventricular rate can be calculated by measuring the time intervals between QRS complexes (the R-to-R intervals). There are instances, such as 2nd and 3rd degree AV block, in which the atrial rate and ventricular rates are different. This is why it is important to know how to determine both atrial and ventricular rates. Rules 1. Count the number of QRS’s in a 6 - second strip, then multiply that number by 10. 2. Determine the time between R-R intervals, then divide that number by 60. For example: 40 ÷ (20 small boxes x 0.04 seconds each) = 50 beats per minute Rules Memorize these numbers: 300, 150, 100, 75, 50 Normal Heart rate for an adult = 60 -100 bpm This means that 3 to 5 large blocks should exist between R – R intervals. Bradycardia = more than 5 large blocks Tachycardia = less than 3 large blocks Figure 8 Let’s Practice with an Example: Figure 9 What is the rate based on Rule #1? If you said 50 bpm…. You are Correct!!! Are the P waves regular or irregular? Are the R-to-R intervals regular or irregular? Are there P-waves in your rhythm strip? Is there a P-wave for each QRS complex? Do all of the P-waves look the same? Is the PR Interval measurement normal? PR = 0.12 – 0.20 seconds Is the PR Interval measurement constant? Is the QRS wide? > 0.10 Is it normal? QRS = 0.08 – 0.10 seconds Or is it narrow? < 0.08 Is the T-wave peaked, inverted or flat? Is the ST segment elevated, depressed or normal? Is the QT Interval < 0.43 seconds? Is there any ectopy present? Let’s try an example….. Figure 10 1. Is the rhythm regular or irregular? Regular 2. Are the P-waves identical? Is there a P-wave for each QRS complex? Yes for both! 3. Is the PR Interval 0.12 – 0.20? Yes, PR = 0.16 4. Is the QRS wide, normal or narrow? Normal QRS = 0.08 5. Is the T-wave peaked, inverted or flat? No, it’s normal 6. Is the ST segment elevated or depressed? No 7. Is the QT Interval < 0.43? Yes, QT Interval= 0.36 And last but not least, is there any ectopy present in this rhythm? NO! And the rhythm is…. Normal Sinus Rhythm Listed below are the cardiac arrhythmias that are almost always associated with death: Atrial Fibrillation Atrial Flutter Ventricular Fibrillation Ventricular Tachycardia 3rd degree AV Block Asystole Atrial Fibrillation Figure 11 Rhythm: Atrial fibrillation is irregular and chaotic; Ventricular rhythm is very irregular Rate: Atrial is > 350 bpm; Ventricular is 120-200 bpm P-waves: not consistent (they are fine and fibrillating) PR Interval: not measurable Atrial Flutter Figure 12 Rhythm: Atrial flutter is usually regular Rate: Atrial is 250-350 bpm Ventricular rate depends on AV conduction P-waves: characterized by “saw tooth” pattern PR Interval: can not be determined; more flutter waves than QRS complexes Ventricular Fibrillation Figure 13 Rhythm: Totally erratic VF Rate: 350-450 bpm P-waves: none QRS: none Ventricular Tachycardia Figure 14 aka “The Widow-Maker” Rhythm: Typically regular, but can be irregular Rate: 100 – 220 bpm P-waves: can be present but have no correlation to QRS complex QRS: > 0.12 seconds with an odd, “tomb –stone” shape 3rd Degree AV Block = Complete Heart Block Figure 15 Rate: 40-60 bpm (narrow QRS and junctional); 20-40 bpm (wide QRS and ventricular) P-waves: normal, but usually more P-waves than QRS’s Asystole Figure 16 In Asystole, there is no rate because the person that belongs to this rhythm is DEAD! Figure 1. (2009). Image retrieved on February 17, 2009 from http://images.google.com/imgres?imgurl=http://www.micardia.c om/images/anatomy-of-the-humanheart.jpg&imgrefurl=http://www.micardia.com/CHF-CongestiveHeart-Failure/Structural-heart-disease-and-mitralprolapses.php&usg=__vAFkAZBOMi2yoKCxSP0R39jzRQE=&h=324 &w=250&sz=48&hl=en&start=288&um=1&tbnid=zVIu6UfvBIh2M:&tbnh=118&tbnw=91&prev=/images%3Fq%3Dblood%2Bflo w%2Bthrough%2Bheart%26ndsp%3D18%26hl%3Den%26sa%3DN %26start%3D270%26um%3D1 Figure 2. (2008). Image retrieved on February 15, 2009 from http://2.bp.blogspot.com/_2MjIeQJj8UM/SPjvLvdNZPI/AAAAAAA AAJA/7KNEAG5TcIY/s1600-h/limb+leads.jpg Figure 3. (2008). Image retrieved on February 15, 2009 from http://2.bp.blogspot.com/_2MjIeQJj8UM/STqKlrU3dpI/AAAAAAA AAa4/anAGFWaQrRQ/s1600-h/ecg08_f8b.jpg Figure 4.(2008). Image retrieved on February 15, 2009 from http://www.szivorvos.hu/english/wp-content/gallery/picturesand-photos-of-heart/electrical-system-of-the-heart.jpg Figure 5. (2004). Image retrieved on February 16, 2009 from http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cardio&par t=A39 Figure 6. (2002). Image retrieved on February 16, 2009 from http://www.a-fib.com/EKGsignal.htm Figure 7. (2006). Image retrieved on February 16, 2009 from http://www.ambulancetechnicianstudy.co.uk/images/ecg_paper1 .gif Figure 8. (2008). Image retrieved on February 17, 2009 from http://ems12lead.blogspot.com/2008/11/large-block-methodfor-heart-rate.html Figure 9. (2006). Image retrieved on March 1, 2009 from http://www.ambulancetechnicianstudy.co.uk/rhythms.html Figure 10. (2008). Image retrieved on March 1. 2009 from http://www.rnlife.com/wp-content/uploads/2008/11/ekgstrip.jpg Figure 11. (2008). Image retrieved on March 1, 2009 from http://www.heartyhealth.com/CV/training/a-fib.html Figure 12. (2004). Image retrieved on March 1, 2009 from http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=cardio&part =A39 Figure 13. (n.d.). Image retrieved on March 1, 2009 from http://www.cs.iupui.edu/~stewarte/N241/vfib.jpg Figure 14. (n.d.). Image retrieved on March 1, 2009 from http://www.cs.iupui.edu/~stewarte/N241/vfib.jpg Figure 15. (2005). Image retrieved on March 1, 2009 from http://www.pacemakerproject.com/assets/img/thirdAV_ecg.jpg Figure 16. (2006). Image retrieved on march 1, 2009 from http://www.ambulancetechnicianstudy.co.uk/images/Asystole.gif Huff, J. (2002). Ecg workout exercises in arrhythmia interpretation. Philadelphia, PA: Lippincott, Williams & Wilkins. Prehospital 12 Lead ECG. (2008). Retrieved on March 10, 2009 from http://ems12lead.blogspot.com/2008/11/large-block-method-forheart-rate.html Smeltzer, S. C. & Bare, B. G. (2004). Brunner & Suddarth’s textbook of medical surgical nursing. (10th ed.). Philadelphia, PA: Lippincott, Williams & Wilkins. Thaler, M. (2003). The only ekg book you’ll ever need. (4th ed.). Philadelphia, PA: Lippincott, Williams & Wilkins. White, K. (2007). Fast facts for adult critical care. Mobile, AL: White Learning Systems. The End !!! Kathy