Blue Lightning
advertisement

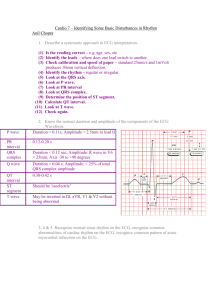
Introduction to EKG for non-EKG Techs By: Adam Arseneault CCT Many Slides Courtesy of : Mícheál P. Macken MD MRCPI And Roneil Malkani MD The Run Down Understanding heart conduction Neurological studies of interest What rhythms to worry about Commonly seen rhythms and conduction abnormalities Question time Cardiac Conduction (Marquette Electronics, 1996 ) Sinoatrial (SA) Node The Sinoatrial Node is the hearts pacemaker Found in the wall of the right atrium at the junction with the superior vena cava Rich vagal and parasympathetic innervation Intrinsic range of firing is 60-100 bpm (French, 2006) Atrioventricular (AV) Node Back-up Pacemaker Located in the wall of the right atrium next to the tricuspid valve Responsible for slowing down conduction from the atria to the ventricles so atrial contraction can occur This slowing lets the atria slightly overfill the ventricles to increase cardiac output and the ventricular pump Rich vagal and parasympathetic innervation Intrinsic rate is 40-60 bpm (French, 2006) Bundle of His (AKA HIS Bundle) Starts just at the bottom of the AV Node to where the Left and Right Bundle Branches fork Located in the right atrium and inter-ventricular septum It is the route of communication between the atria and ventricles Intrinsic rate of 40-45 bpm (French, 2006) Right and Left Bundle Branches Left Bundle Branches Right Bundle Branch Conducts to the left ventricle Conducts to the right ventricle Intrinsic rate is 40-45 bpm (French, 2006) Purkinje System Made up of individual cells just beneath the endocardium These cells initiate the ventricular depolarization cycle Located in the ventricles Intrinsic rate 20-40 bpm (French, 2006) Cardiac Conduction (Marquette Electronics, 1996 ) Conduction in Motion What is an EKG? Basics: Waveforms are representations of the electrical activity created by depolarization of the atria and ventricles With an EKG we can measure the rate and regularity of heartbeats, as well as the size and position of the chambers, the presence of any damage to the heart, and the effects of drugs or devices used to regulate the heart, such as a pacemaker. What is an EKG? 12-lead ECG - 10 electrodes required to produce 12lead ECG. - – Electrodes on all 4 limbs (RA, LA, RL, LL) - – Electrodes on precordium (V1–6) - Monitors 12 leads (V1–6), (I, II, III) and (aVR, aVF, aVL) - Allows interpretation of specific areas of the heart - – Inferior (II, III, aVF) - – Lateral (I, aVL, V5, V6) - – Anterior (V1–4) What is an EKG? What is an EKG? P Wave (Atrial Depolarization) QRS Complex (Rapid Ventricular Depolarization) T Wave (Ventricular Repolarization) (Wagner, 2006) Depolarization and Repolarization Depolarization when a cell membrane's charge becomes positive in order to generate an action potential. Caused by positive sodium and calcium ions going into the cell (concentration gradient) Repolarization (re-negative) when a cell membrane's charge returns to negative after depolarization. Caused by positive potassium ions moving out of the cell. What is an EKG? 1mm (small square) = 40 ms 5mm (big square) = 200 ms Methods for measuring heart rate For regular rhythms: Rate = 300 / number of large squares in between each consecutive R wave For very fast rhythms: Rate = 1500 / number of small squares in between each consecutive R wave For slow or irregular rhythms: Rate = number of complexes on the rhythm strip x 6 (this gives the average rate over a ten-second period) What is an EKG? PR Interval QRS Interval QT Interval Interval Norms P-Wave PR Interval Time from beginning of the P wave to the beginning of the QRS complex (onset of ventricular depolarization) Normal range is from 120 ms – 200 ms Atrial contraction begins in the middle of the P wave and continues throughout the PR interval Corresponds to the delay necessary for the ventricles to fill after atrial contraction The atrial repolarization wave (electrical impulse) is usually hidden by the QRS complex QRS Complex Time it takes for the depolarization of the ventricles Norms – 40 ms to 120 ms measured from the initial deflection of the QRS from the isoelectric line to the end of the QRS complex. R-wave point when half of the ventricular myocardium has been depolarized RS line activation of the posteriobasal portion of the ventricles Ventricular Depolarization Ventricular depolarization requires normal function of the right and left bundle branches. A block in either the right or left bundle branch delays depolarization of the ventricles, resulting in widening QRS Ventricular contraction begins at about half-way through the QRS complex and continues to the end of the T-wave. Pumping of blood begins when ventricular pressure exceeds aortic pressure, causing the semi lunar valves to open. This is normally at the end of the QRS complex and start of ST segment. (Molson Medical Informatics Project, 2000) ST Segment Period from the end of ventricular depolarization to the beginning of ventricular repolarization Although the ST segment is isoelectric, the ventricles are actually contracting Elevated or depressed is a hallmark sign of ischemia, CAD or impending MI (STEMI) Norm 80 ms to 120 ms (Molson Medical Informatics Project, 2000) QT Interval Normally 340 ms to 430 ms Measure from the beginning of the Q wave to the end of the T wave Represents the total duration of electrical activity of the ventricles Prolonged QT is associated with an increased risk of ventricular arrhythmias, especially torsades de pointes QTc is prolonged if > 440ms in men or > 460ms in women QTc > 500 is associated with increased risk of torsades de pointes QTc is abnormally short if < 350ms A useful rule of thumb is that a normal QT is less than half the preceding RR interval T Wave Corresponds to the rapid ventricular repolarization Normally rounded and positive Most labile wave in the EKG U Wave Thought to represent repolarization of the purkinje fibers Not always seen Prominent U waves are most often seen in hypokalemia, but may be present in hypercalcemia, thyrotoxicosis, or exposure to digitalis, or epinephrine Telemetry Monitoring Rate per minute Examine R to R regularity Check P waves Measure PR Interval Determine if each P wave is followed by a QRS complex Examine the QRS Examine the QT Interval (Wagner, 2006) Normal Cardiac Rhythm Rate: 60-100 bpm Regular rate and rhythm PR Interval between 120-200 ms QRS Interval between 40-120 ms QT Interval between 340-430 ms Sinus Rhythm Rate: 60-100 bpm Regularity: Regular P-Waves: Regular and 1:1 ratio with QRS PR Interval: PR 120-200 ms Sinus Bradycardia Rate: <60 bpm Regularity: Regular P-Waves: Regular and 1:1 ratio with QRS PR Interval: PR 120-200 ms Sinus Tachycardia Rate: >100 bpm; usually under 170 bpm Regularity: Regular P-Waves: Regular and 1:1 ratio with QRS PR Interval: PR 120-200 ms Sinus Arrhythmia Rate: Any sinus rate Regularity: Irregular P-Waves: Regular and 1:1 ratio with QRS PR Interval: PR 120-200 ms EKG Abnormalities During Partial Seizures in Refractory Epilepsy Fifty-one seizures in 43 patients with intractable partial epilepsy Cardiac rhythm and conduction abnormalities are common during seizures, particularly if they are prolonged or generalized, in intractable epilepsy. These abnormalities may contribute to SUDEP. Nei et al, Epilepsia, 2000 EEG and ECG in Sudden Unexplained Death in Epilepsy 21 patients with SUDEP compared with previous study of 43 patients with refractory partial epilepsy – studied ECG changes Ictal max HR was significantly higher in SUDEP patients than in controls (mean 149 bpm vs 126 bpm) Ictal cardiac repolarization or rhythm abnormalities 56% in SUDEP vs 39% in controls: not significant Nei et al, Epilepsia, 2004 Ictal asystole (IA) =preventable cause of sudden unexplained death in Epilepsy Compared heart rate (HR) characteristics of IA patients to a group of patients with vasovagal (benign, not seizure-related) asystole. IA was seen in 8 patients, all with temporal lobe epilepsy. No statistical difference was found in: – duration of asystole, bradycardia, and baseline HR characteristics Only significant difference: higher HR acceleration post-asystole in the controls. Schuele et al, Epilepsia, 2008 Arrhythmias Encountered in Neurological Conditions (Stroke, Seizures, etc.) Atrial Ventricular Bradycardia • Supraventricular tachycardias Ectopic ventricular beats • Multifocal ventricular tachycardias • Torsades de pointes • Ventricular fibrillation Atrial flutter Atrial fibrillation Possible Mechanisms: Altered parasympathetic/vagal activity Altered sympathetic activity Imbalance between these two arms of the autonomic nervous system Increased circulating catecolamines Premature Atrial Contractions These complexes originate in the atria They often originate from ectopic pacemaker sites within the atria which results in an abnormal P wave The complex occurs before the normal beat is expected, and followed by a pause Premature Atrial Contractions Rate: Underlying rhythm Regularity: Irregular with PAC's; Compensatory Pause P-Waves: Ectopic P-wave; Differs from Sinus P wave PR Interval: Differs from underlying Sinus P wave Supraventricular Tachycardia Regularity: Regular Rate: 140 – 220 bpm P-Waves: Usually blocked by preceding T wave QRS: Generally normal Usually starts and stops suddenly Atrial Flutter Rate: Atrial: 240-440 bpm; Ventricular varies Regularity: Atrial rate regular; Ventricular rate from 2:1 to 8:1 Atrial flutter is characterized by "sawtooth" atrial activity and a conduction ratio to the ventricles of 2:1 to 8:1 Caused by a reentry circuit located in the right atrium Check patients cardiac history, if any Atrial Fibrillation Rate: Can vary Regularity: Irregular P-Waves: No discernible P-wave present This is the most common sustained cardiac arrhythmia Characterized by an undulating baseline replacing P waves and an irregularly irregular ventricular response Check patients cardiac history, if any Premature Ventricular Contraction A PVC is a depolarization that arises in either ventricle before the next expected sinus beat altering the normal sequence of depolarization The two ventricles depolarize sequentially instead of simultaneously Conduction moves slowly and this results in a widened QRS complex (greater than 120 ms) Three or more PVC's in a row is considered a run of Ventricular Tachycardia If it lasts for more than 30 seconds it is designated sustained VT (French, 2006) Premature Ventricular Contraction Rate: Underlying rhythm Regularity: Irregular P-Waves: Underlying rhythm PR Interval: Underlying rhythm QRS: Severely different from other beats, >120 ms Ventricular Tachycardia Rate: >100 bpm to <220 bpm Regularity: Generally Regular; Can be Irregular QRS Interval: >120 ms Treatment: If patient is sleeping – wake them up and see if they are responsive and whether rhythm terminates. Also check whether pt. has AICD If neither – call Code! Torsades de Pointes Torsades de Pointes Polymorphic ventricular tachycardia (PVT) is a form of ventricular tachycardia in which there are multiple ventricular foci with the resultant QRS complexes varying in amplitude, axis and duration. The most common cause of PVT is myocardial ischaemia. Torsades de pointes (TdP) is a specific form of polymorphic ventricular tachycardia occurring in the context of QT prolongation; it has a characteristic morphology in which the QRS complexes “twist” around the isoelectric line. For TdP to be diagnosed, the patient has to have evidence of both PVT and QT prolongation. Ventricular Fibrillation Rate: Very Rapid; too unorganized to count Regularity: Irregular; No normal QRS; Waveform varies in size and shape; No Pwaves; No T-waves Treatment is always immediate unsynchronized defibrillation Ventricular Fibrillation Ventricular Fibrillation is a rhythm in which multiple areas within the ventricles are erratically depolarizing and repolarizing There is no organized depolarization, therefore the ventricles do not contract as a unit The myocardium is quivering - There is no cardiac output This is the most common arrhythmia seen in cardiac arrest from ischemia or infarction. The rhythm is described as coarse or fine VF. Coarse VF indicates recent onset of VF. Prolonged delay without defibrillation results in fine VF and eventually asystole Treatment is always immediate unsynchronized defibrillation Asystole No Conduction Asystole represents the total absence of ventricular electrical activity Since depolarization does not occur, there is no ventricular contraction This may occur as a primary event in cardiac arrest, or it may follow VF or pulseless electrical activity (PEA). Treatment: Immediate Transient Asystole Asystole can also be transient, a few seconds up to 1 minute or longer, due to vagal hyperactivity Sleep apnea/Snoring during sleep Valsalva maneuver During seizures : Ictal asystole Medullary centers in brainstrem Valsalva reflex Other causes Ancillary Information • Junctional Rhythms/beats • AV Blocks • First, Mobitz I and II, Third degree • WPW • Brugada • Electronic Pacer Junctional Escape Rhythm Rate: 40-60 bpm Regularity: Regular P-Waves: They will be inverted, and may appear before or after the QRS complex, or they may be absent, hidden by the QRS PR Interval: If Present PR <120 ms Premature Junctional Contraction Rate: Underlying rhythm Regularity: Irregular P-Waves: They will be inverted, and may appear before or after the QRS complex, or they may be absent, hidden by the QRS PR Interval: If Present PR <120 ms First Degree AV-Block Regularity: Regular Rate: Underlying rhythm P-Waves: Regular and 1:1 ratio with QRS PR Interval: Constant and prolonged PR Interval, >0.20 sec Second Degree AV-Block; Type 1Wenckebach Regularity: Irregular Rate: Underlying rhythm P-Waves: Regular PR Interval: PR gradually elongates until a dropped beat which leads to a reset This is usually benign and due to increased vagal activity Second Degree AV-Block; Mobitz Type 2 Rate: Underlying rhythm Regularity: Irregular P-Waves: Regular PR Interval: P-waves march but not all conducted This block is bad because it originates below the AV node, the escape rhythm is too slow Treatment is a pacemaker Third Degree AV-Block; Complete Heart Block Rate: Underlying rhythm P-Waves: Regular but not related to QRS A total lack of conduction through the AV node This conduction defect is dangerous and may progress to ventricular standstill Treatment is an artificial pacemaker Wolff-Parkinson-White Syndrome Short PR interval (< 120ms) Broad QRS (> 100ms) A slurred upstroke to the QRS complex (the delta wave) Pre-excitation refers to early activation of the ventricles due to impulses bypassing the AV node via an accessory pathway In WPW the accessory pathway is often referred to as the Bundle of Kent, or atrioventricular bypass tract Lifeinthefastlane.com Can cause tachyarrhythmia Wolff-Parkinson-White Syndrome Bundle of Kent Accessory Pathway Brugada Syndrome Note the pattern resembling a right bundle branch block, the P-R prolongation and the ST elevation in leads V1-V3 Brugada is a recently found arrhythmia that can lead to ventricular fibrillation, also may be inherited. Brugada.org Pacemaker Rhythms If a patient has a pacemaker you may see spikes representing the electrical activity from the pacemaker You could see a “spike” preceding a wide QRS when ventricular pacing Or a “spike” preceding P wave when atrial pacing Ventricular Pacemaker Rhythm Atrial Pacemaker Rhythm Atrial and Ventricular Pacing Left-sided Brain Hemorrhage Causing ST Segment Elevation Introduction to EKG for non-EKG Techs By: Adam Arseneault CCT Many Slides Courtesy of : Mícheál P. Macken MD MRCPI And Roneil Malkani MD